Many patients with advanced cancer develop various symptoms that can limit the effectiveness of pain treatment and significantly impair quality of life [4]. A previous report indicated that pain treatment was inadequate for 14% of patients [4].
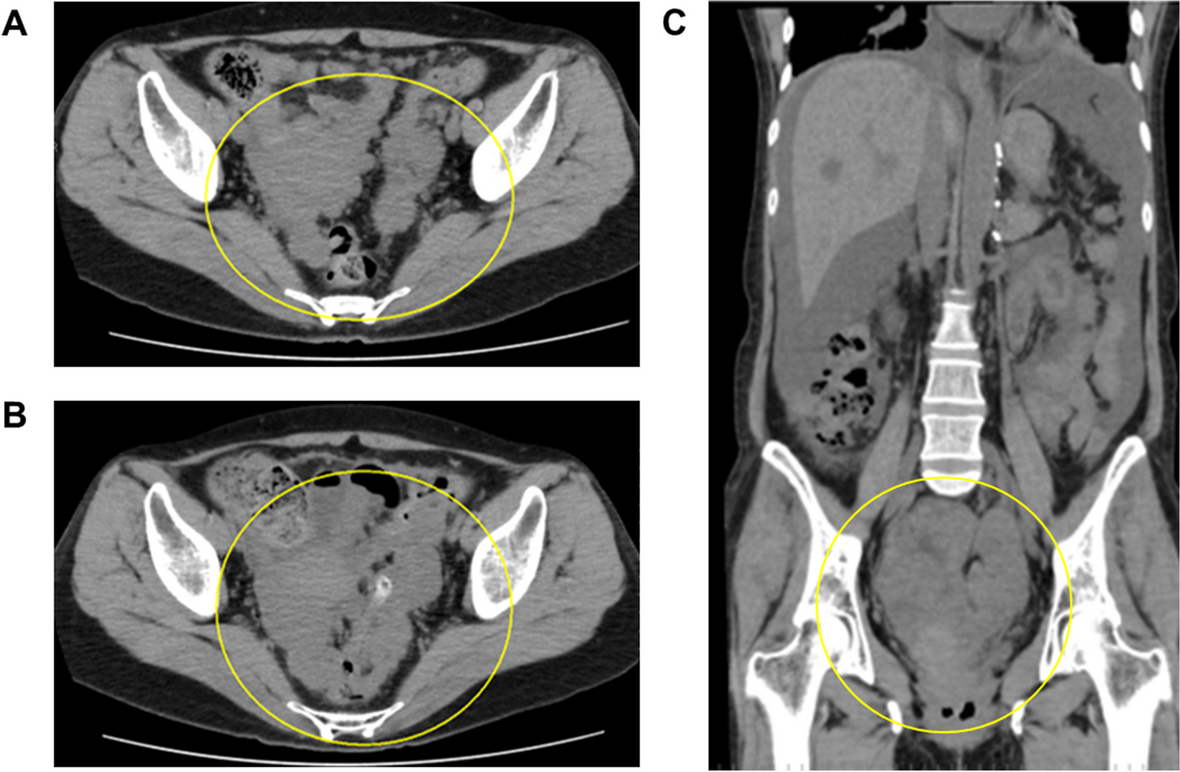
To date, there have been no reports of continuous sacral epidural ethanol injections specifically for anal pain resulting from intraperitoneal dissemination of malignant pheochromocytomas. Pheochromocytomas are rare catecholamine-secreting tumors with an incidence of approximately 2–8 per million adults, of which approximately 10% are malignant, and pain in these patients is typically caused by direct tumor invasion and multiple bone metastases [5].
Rectal cancer and peritoneal tumor dissemination often cause perineal and anal pain, which is highly resistant to opioids [2]. Opioids are generally effective for C-fiber-derived pain, but perineal and anal pain caused by contact with the tumor is thought to be primarily mediated by Aδ fibers [3, 6]. This type of pain often worsens during defecation or when sitting. Intrathecal phenol block is effective for pain management of these perineal pains [1, 2, 6]. However, its applicability is limited because it tends to cause vesicorectal and lower limb movement disorders, often requiring stoma extension and urinary catheterization [1, 5, 7].
A one-shot sacral epidural ethanol injection has been reported as a nerve-destructive method [8]. However, it has been reported that the pain relief effect of a single administration of ethanol is often inconsistent, with many patients requiring repeated blocks.
In contrast, the continuous sacral epidural ethanol block is a nerve destruction technique first reported by a Japanese anesthesiologist [3], blocking only the sensation at the S4 and S5 levels. This procedure can be performed safely by first administering a continuous dose of a local anesthetic [9].
In recent years, reports have highlighted the effectiveness of continuous sacral epidural blocks for managing anal pain resulting from rectal invasion by prostate cancer [9] and rectal tenesmus associated with cervical cancer [10].
Another advantage is that nerve destruction can be performed only in the S4 and S5 regions by administering a small amount of ethanol continuously through the epidural catheter. This method can provide pain relief without causing motor disorders of the lower limbs, bladder, or rectum.
Thus, sacral epidural continuous ethanol infusion therapy is considered appropriate for severe pain that is not relieved by the administration of analgesics such as opioids and NSAIDs [10].
The procedure for a continuous sacral epidural ethanol block is as follows [3]. After inserting the catheter into the sacral epidural space, continuous local anesthetic administration begins at 2 mL/h for approximately 12 h, reducing the infusion rate if urinary dysfunction or lower extremity sensorimotor nerve block occurs. If neurological findings such as dysuria or sensory loss in the lower extremities are observed, the continuous dosage is decreased by 0.5 mL/h. This sustained dose serves as a guideline for a safe, sustained dose of absolute ethanol.
Before continuous administration, the position of the catheter tip is confirmed by X-ray and contrast agent administration. After positioning is confirmed, 1.5 mL of absolute ethanol is slowly administered over approximately 5 min for nerve disruption, followed by a continuous ethanol infusion at the same rate as the initial anesthetic dose.
The administration was continued for 2 h, and the patient was paused for 1 h to check for changes in neurological findings. During the continuous administration of ethanol, the patient was allowed to assume a comfortable position on the bed. Similarly, during the 1-h break, there were no restrictions on the patient’s position, and they were encouraged to remain comfortable in bed.
However, given the risk of falling, it is advisable to limit patient ambulation, allowing movement only to a portable bedside toilet during the break. The above 3-h treatment was considered to be one course, which ends after 1–3 courses [3, 9, 10]. After the ethanol injection, the patient was allowed to walk if they did not feel uncomfortable or unsteady.
Although sacral epidural ethanol injection therapy carries a risk of vesicorectal disorders or lower extremity movement disorders, the incidence of these complications is generally considered to be low [3, 10]. This is because the optimal dosage can generally be estimated from a test block, and this dosage is believed to be unlikely to cause bladder or rectum disorders or neurological symptoms in the lower limbs. However, if symptoms such as bladder or rectum dysfunction or sensory loss in the lower limbs are observed, ethanol administration should be discontinued.
The advantage of this method is that it is a relatively simple procedure, as it can be performed at the bedside as well.
This method involves indwelling a catheter in the sacral epidural space and continuously administering a small amount of absolute ethanol to block sensation only in the perineal and anal areas and achieve pain relief. It is mainly suitable for patients who are able to excrete on their own because it can block the perception of S4 and S5 regions without affecting excretory or motor functions.
We report a case in which sacral epidural ethanol injection therapy was successful in managing anal pain that worsened while standing in a patient with multiple metastases from malignant pheochromocytoma. Given that sacral epidural ethanol injection carries a relatively low risk of complications, it is recommended for anal pain that is unresponsive to standard analgesic treatment.









留言 (0)