HCC is a common malignant tumor that originates from malignant cells in liver tissue [5]. It is usually divided into two types: primary HCC and metastatic HCC. Primary HCC refers to tumors originating within the liver, while metastatic HCC is a metastatic tumor formed by the spread of cancer from other parts of the liver [6]. The incidence rate of HCC is very high worldwide, especially in East Asia, where one of the most prevalent malignant tumors is HCC. HCC can be treated in a number of ways, including as liver transplantation, chemotherapy, radiation, targeted therapy, and surgical excision [7]. Among these treatment methods, surgical resection is widely considered one of the main methods for treating HCC, especially suitable for early stage HCC patients. Surgical resection can achieve complete cure by removing tumors and surrounding healthy tissues. However, HCC surgery is a complex surgical process for patients, which requires consideration of factors such as the patient’s liver function, surgical resection range, and preserved liver capacity [8]. In HCC surgery, SABT has been widely used as a blood transfusion method. SABT is the process of collecting and preserving the patient’s own blood before surgery, and then infusing it to the patient during the surgery process. Compared with allogeneic blood transfusion, SABT has the following advantages: it avoids the risk of immune reactions, infectious disease transmission, and blood type mismatch that may be caused by allogeneic blood transfusion; It reduces the demand for allogeneic blood, reduces the burden and cost of allogeneic transfusion; It provides the patient’s own blood components, which may help maintain stable blood circulation and reduce the occurrence of postoperative complications [9]. However, despite the potential advantages of SABT in HCC surgery, there is relatively little research on its application in HCC surgery. Especially for the specific mechanisms of SABT on pro-inflammatory cytokine changes and liver function recovery, there is insufficient understanding. The changes in pro-inflammatory cytokines play an important regulatory role in HCC surgery, and have a significant impact on postoperative inflammatory response and liver damage. Therefore, studying the mechanism of the application of SABT in HCC surgery can better understand its impact on inflammatory response and liver function, and provide better guidance for postoperative recovery and prognosis of patients.
4.1 Blood routine changes
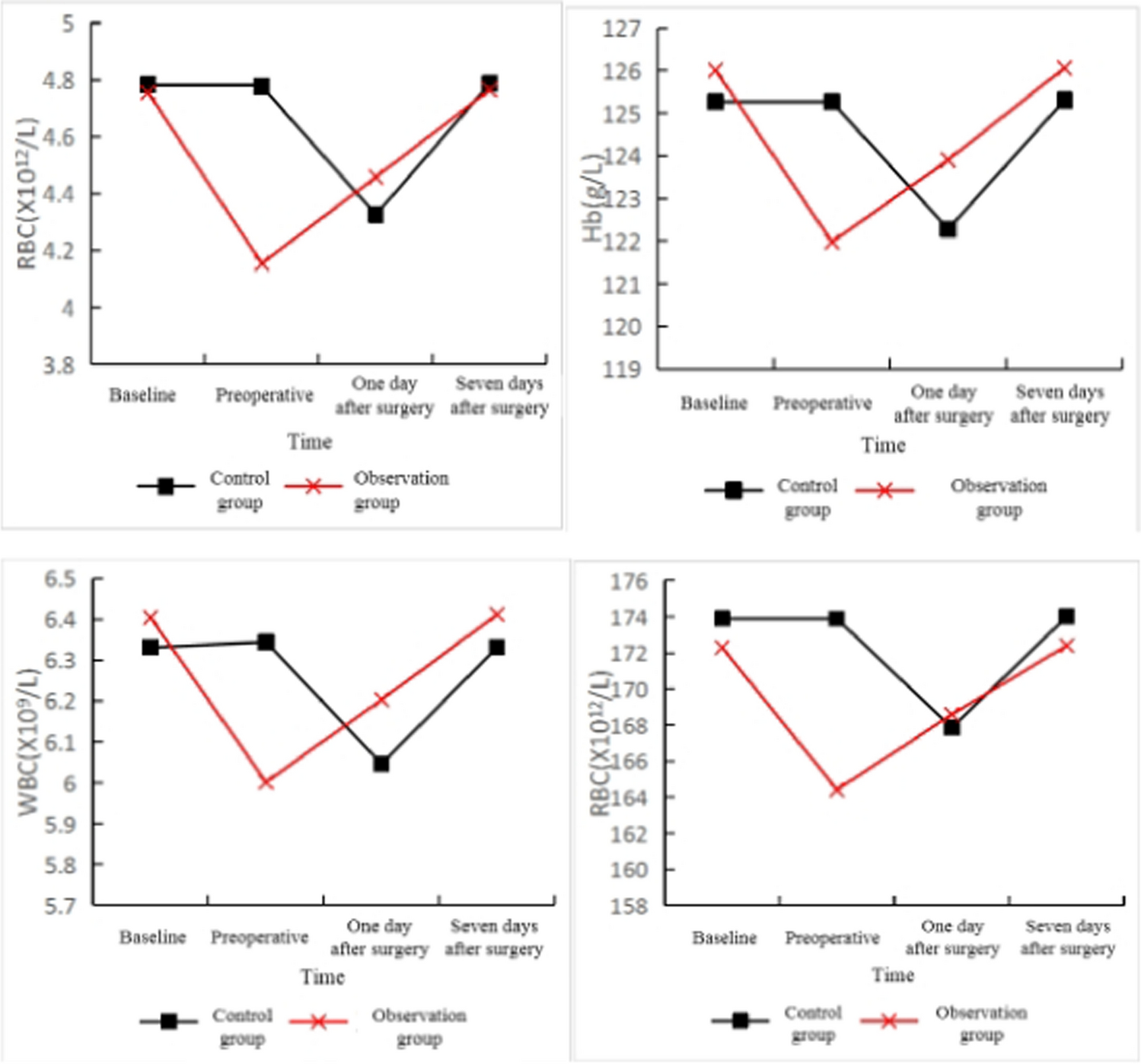
The levels of RBC and Hb reflect the patient’s anemia status, and massive bleeding is a common occurrence during HCC surgery; Therefore, evaluating the patient’s anemia level before surgery, especially whether the Hb level is below the normal range, can help doctors determine the surgical risk and postoperative recovery. Low hemoglobin levels may require preventive blood transfusion or other treatment measures to ensure the safety of the surgery and the patient’s postoperative recovery. The white blood cell count reflects the patient’s immune status and degree of inflammatory response. In HCC surgery, there may be a risk of infection after surgery, and an increase in white blood cell count can indicate the presence of infection or inflammatory response in the patient [10]. Platelets are an important component of blood coagulation. HCC surgery involves liver resection or puncture, which may lead to abnormal coagulation function and the risk of postoperative bleeding. By monitoring platelet count, it is possible to evaluate the patient’s coagulation function status, promptly detect thrombocytopenia, and take necessary preventive measures, such as infusion of platelet concentrate, to ensure postoperative hemostatic effect and patient safety.
The results of this study showed that the CG and the OG showed different trends in blood routine indicators; The CG showed no significant changes in baseline and preoperative blood routine indicators, but showed a downward trend on the day after surgery, and then returned to normal levels seven days after surgery. The OG showed a significant decrease in preoperative blood routine indicators, and then gradually increased one day and seven days after surgery, returning to normal levels. In addition, there was no SD between the CG and the OG at baseline, 1 day after surgery, or 7 days after surgery (p > 0.05), and the blood routine index levels in the preoperative OG were markedly below those in the CG. A study on 27 pregnant women with SABT found that SABT significantly improved Hb, Hct, and PLT levels, with statistically SD compared to the CG [11]. Another study on the application of SABT in elective surgery showed that the red blood cell count and hemoglobin concentration after SABT markedly exceeded those in the CG (P < 0.05) [12]. Similar to previous studies, the results of this study also suggest that SABT has better blood recovery ability. The OG had significantly lower preoperative indicators than the CG, but slightly higher than the CG one day after surgery, with no statistically SD (p > 0.05). The possible reasons for the analysis are as follows: storage autologous blood transfusion is the process of storing the patient’s own blood and then administering it during surgery. Due to the use of one’s own blood, the occurrence of immune and inflammatory reactions may be reduced. Therefore, the blood routine indicators in the preoperative OG have already decreased, which may be related to cell damage and changes in blood composition caused during the preoperative blood collection and storage process. The increase in indicators one day and seven days after surgery may be due to autologous blood transfusion providing the necessary blood cells and platelets in one’s own blood, promoting the recovery of hematopoietic and coagulation functions.
4.2 Changes in pro-inflammatory cytokines
IL-1, IL-6, and TNF-α are important inflammatory factors. IL-1 is an early inflammatory mediator involved in various biological processes, such as immune regulation, inflammatory response, and cell proliferation; In HCC surgery, surgical trauma can activate inflammatory reactions, leading to an increase in the release of IL-1. The increase of IL-1 may promote the occurrence of inflammatory reactions, thereby affecting the recovery and repair process of liver tissue. In addition, IL-1 is also associated with tumor growth and metastasis, and its excessive production may have a negative impact on the prognosis of HCC. IL-6 is an early inflammatory factor that is mainly regulated by stimuli such as tissue damage, inflammation, and cellular stress; In HCC surgery, surgical trauma and tumor resection may lead to the activation of inflammatory response, which in turn promotes the increase of IL-6 release; The elevation of IL-6 can be regarded as an indicator of inflammatory response, reflecting the degree of inflammatory response and tissue damage during the surgical process [13]. TNF-α is involved in regulating inflammatory response, cell apoptosis, and immune regulation. In HCC surgery, surgical trauma and tumor tissue destruction may lead to an increase in TNF-α release. The increase in TNF-α may trigger inflammatory response and cell damage, thereby affecting the recovery and repair of liver tissue.
The pro-inflammatory cytokines IL-1, IL-6, and TNF-α levels in this study demonstrated a tendency of initially rising and then falling prior to surgery, one day following surgery, and seven days following surgery. To be more precise, on the first and seventh postoperative days, the levels of IL-1, IL-6, and TNF-α in the OG were significantly lower than those in the CG (P < 0.05). However, there was no SD in these values between the preoperative CG and the OG (P > 0.05). The reasons for the analysis are as follows: On the first day after surgery, the levels of IL-1, IL-6, and TNF-α in the OG were markedly below those in the CG. This may be due to the application of SABT, which reduces the immune and inflammatory reactions that may be triggered by allogeneic blood transfusion, thereby reducing the production of these inflammatory factors. In addition, the OG may benefit from the protective effects of immune cells and cytokines in autologous blood transfusion, which can help alleviate postoperative inflammatory reactions [14]. On the 7th day after surgery, the levels of IL-1, IL-6, and TNF-α in the OG were still markedly below those in the CG. This may indicate that SABT can help regulate the duration and degree of postoperative inflammatory response. The OG may have experienced fewer inflammatory reactions in the early postoperative stage, thus reaching lower levels of cytokines by 7 days after surgery. In contrast, the CG may require longer time to regulate and restore inflammatory reactions [15].
4.3 Recovery of liver function
This study utilized MELD, HAF, and PVF to evaluate the recovery of liver function. The MELD score is on the ground of indicators such as serum bilirubin, serum creatinine, and international standardized ratio (INR). By calculating a score, a higher MELD score indicates poor liver function and correspondingly increases the risk of surgery. HAF refers to the blood flow of the hepatic artery, which reflects the blood supply of the liver. In HCC surgery, the blood supply of the hepatic artery is closely related to the metabolic activity and function of the liver. A lower hepatic artery flow may indicate insufficient blood supply to the liver, which may affect its metabolism and function. PVF reflects the blood flow of the liver, and in HCC surgery, preoperative evaluation of changes in portal vein blood flow is of great significance for predicting postoperative liver function and prognosis. Portal vein blood flow is the main channel for the liver to receive and clear blood, which is crucial for liver metabolism and function. Reduced portal vein blood flow may indicate impaired or compressed liver function.
This study found that there was no change in MELD scores between the OG and the CG prior to surgery (P > 0.05). Prior to surgery, there was no difference in HAF between the OG and the CG (P > 0.05); however, on the first and seventh postoperative days, the OG's MELD scores were considerably lower than the CG's (P < 0.05); prior to surgery, there was no difference in HAF between the OG and the CG (P > 0.05). On the 1st and 7th day after surgery, the HAF in the OG markedly exceeded that in the CG (P < 0.05); There was no SD in PVF between the OG and the CG before surgery (P > 0.05); On the first day after surgery, the PVF of the OG was markedly below that of the CG (P < 0.05); There was no SD in PVF between the OG and the CG 7 days after surgery. It is evident from the study results that have been supplied that there are variations in MELD scores, HAF, and PVF between the OG and the CG. The following is an explanation for the possible reasons for these differences: (1) The MELD score in the postoperative OG was markedly below that in the CG, indicating a more significant protective effect of SABT on liver function. SABT may reduce the burden and damage to the liver after surgery, promote rapid recovery of liver function, and thus reduce MELD scores. Allogeneic blood transfusion in the CG may trigger immune responses, including blood type mismatch and immune system activation, which may lead to activation of inflammatory reactions and cell damage, and have adverse effects on the liver [16]. The use of SABT using the patient’s own blood can avoid immune reactions related to allogeneic transfusion, thereby reducing immune activation and inflammatory damage to the liver. In addition, autologous blood transfusion collects and stores the patient’s blood before surgery, maintaining the integrity of cells and cytokines in the blood. Infusing one’s own blood can provide sufficient oxygen and nutrients, reduce the occurrence of liver ischemia–reperfusion injury, and help protect the integrity and function of liver cells. (2) On the 1st and 7th postoperative days, the HAF of the OG markedly exceeded that of the CG, which may be related to the blood supply of the liver by SABT. Autologous blood transfusion may help maintain the blood flow of the hepatic artery, provide sufficient oxygen and nutrients, and promote liver metabolism and functional recovery. Autologous blood transfusion can maintain postoperative blood volume and circulatory stability. During the surgery, there may be a large amount of blood loss, leading to insufficient blood volume and decreased circulating blood flow, which affects the supply of hepatic artery blood flow. By infusing one’s own blood, it is possible to replenish blood volume in a timely manner, maintain hemodynamic stability, ensure sufficient blood perfusion to the liver, and promote the maintenance of hepatic artery blood flow. The blood provided by autologous blood transfusion can maintain appropriate blood oxygenation and oxygen supply, and the liver is a highly metabolic organ with a high demand for oxygen. By infusing one’s own blood, it can ensure sufficient oxygen content in the blood to meet the oxygen needs of the liver, thereby promoting normal metabolism and functional recovery of liver cells [17]. (3) After HCC surgery, postoperative hemodynamics may change, and there may be significant blood loss and fluid replacement during the surgery process; This may have an impact on blood circulation, and postoperative hemodynamic changes may include adjustments in blood volume, changes in vascular resistance, and adjustments in circulating blood flow; These changes may have a certain impact on portal vein blood flow, leading to a decrease in PVF in the OG one day after surgery. On the 1st day after surgery, the PVF of the OG was markedly below that of the CG, while there was no SD among the participants in this experiment on the 7th day after surgery; This may be due to postoperative hemodynamic changes and metabolic recovery of the liver. The postoperative inflammatory response and liver tissue repair process may have a certain impact on portal vein blood flow. The decrease in PVF in the OG on the first day after surgery may reflect the postoperative hemodynamic changes and liver recovery process, but there was no SD in PVF between the OG and the CG on the seventh day after surgery; This may mean that the blood flow in the liver has returned to a relatively normal level.






留言 (0)