The incidence of gout and CRC has been increasing with economic development and lifestyle changes. Nevertheless, classical epidemiologic studies face challenges in explaining the causal sequence of exposure factors and disease outcomes due to confounding variables. MR analysis offers a straightforward and easily applicable approach that serves to minimize bias, improve comparability, and mitigate the impact of confounding variables. In this study, using GWAS data of SNPs, we discovered for the first time through MR analysis that the risk of CRC gradually decreased with the accumulation of gout, whereas OS and CSS of CRC were enhanced. These findings indicate a mitigating effect of gout on CRC outcomes.
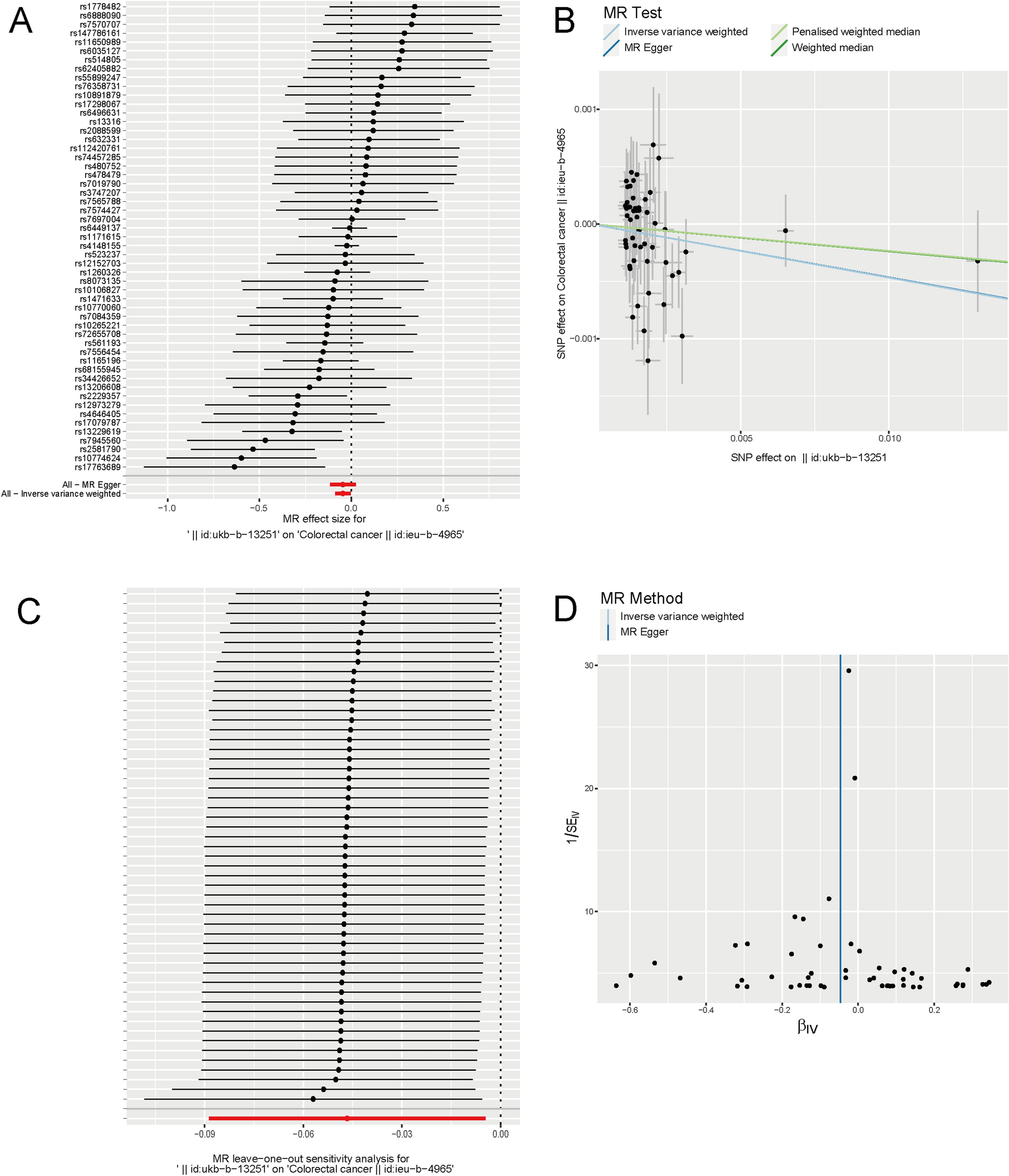
Initially, gout was defined as the exposure factor, and CRC as the outcome. Analysis conducted using the MR approach revealed a gradual decrease in the risk of CRC with increasing gout levels (IVW approach: p = 0.030, beta = − 0.047, OR = 0.954, 95% CI = 0.915–0.995), indicating a potential protective role of gout against CRC. This is consistent with the results of a recent Mendelian randomization study on serum uric acid levels and CRC [26]. In a study conducted by Slobodnick et al., individuals diagnosed with gout demonstrated a lower prevalence of CRC, as confirmed through colonoscopy, compared with those with osteoarthritis but without gout. This observation indicates a potential protective effect of gout against CRC [19]. In addition, Kwon et al., in a study of 9920 CRC patients and 39,680 controls, found a slight decrease in the risk of CRC among patients with gout under the age of 65 years (95% CI, 0.70–0.95; p = 0.009) [20]. Various factors, including pharmaceutical interventions and the antioxidative properties associated with uric acid, may have contributed to this finding. Uric acid, the main etiological factor in gout development, exhibits antioxidant properties that help reduce the generation of reactive oxygen species resulting from prolonged inflammation. These properties also contribute to the preservation of bone metabolism, nerve function, and cardiovascular [27,28,29]. Wang et al. showed that uric acid accumulation plays a significant role in activating TAK1, inducing DNA damage-induced MICA/B expression, and enhancing anti-tumor immune responses [30]. Furthermore, at the onset of gout, there is an enrichment of immune cells and an upregulation of systemic inflammatory factors, including CD8+ T cells, NK cells, and inflammation-related chemokines. These processes may facilitate the body's removal of tumor cells [21].
However, numerous drugs are available for treating gout, such as colchicine (COL), indomethacin (IND), and allopurinol (ALP). COL, a naturally occurring alkaloid present in the Liliaceae family, has demonstrated efficacy in inducing cell death in SW480 cells at low doses, indicating potential antitumor properties [31]. IND is a nonsteroidal anti-inflammatory drug [32]. A previous study reported that the combination of IND and vitamin D substantially decreased the incidence and severity of colon cancer [33]. ALP is an organic compound mainly employed as a uric acid-lowering agent. According to a meta-analysis, ALP exhibits beneficial anti-colorectal cancer activity [34]. Consequently, subsequent pharmacological interventions may exert a degree of anti-tumor efficacy. However, additional clinical cohort studies are required to substantiate these findings.
It is noteworthy that certain studies have reported an association between hyperuricemia, gout, and an increased risk of colorectal cancer (CRC) [17, 18, 35], findings that contradict our results. This discrepancy may be attributed to variations in research methodologies. On the one hand, data selection is the basis of research. If the number of SNPs included in the study is different, different analysis results may result. For example, in the Mendelian randomization study on the effect of uric acid on CRC, Zhou et al. used 26 SNPs [35], while in the study of Leed et al., only 14 SNPs were included in the initial MR analysis and only 3 SNPs in the second MR analysis [26]. The number and representativeness of the selected SNPs may affect the robustness and reliability of the results. On the other hand, Mendelian randomization employs SNPs as instrumental variables, which can significantly mitigate bias in causal inference and yield more robust results. Conversely, observational studies are often susceptible to numerous confounding factors, potentially resulting in instability and bias in their outcomes.
To provide additional evidence supporting the influence of gout on CRC, further investigation into the effect of gout on survival in CRC was conducted using MR. As determined by the IVW approach, our results were consistent with previous studies, demonstrating that the presence of gout exerted a cumulative positive impact on the survival outcomes of patients with CRC, including OS and CSS (OS: p = 0.022, beta = − 8.453, OR = 0.0002, 95% CI = 1.560 × 10−7–0.292; CSS: p = 0.013, beta = − 10.726, OR = 2.200 × 10−5, 95% CI = 4.660 × 10−9–0.104).
This study provides numerous advantages. First, MR was employed to alleviate data bias and eliminate the influence of confounding variables. Second, not only is the correlation between gout and the incidence of CRC investigated but also the effect of gout on survival in patients with CRC is examined, thereby enhancing the validity of the findings of this study. However, this study has certain limitations, particularly the exclusive inclusion of samples from Europe, which limits our ability to determine potential variations across racial groups. In addition, the precise mechanism by which gout decreases the incidence of CRC and improves survival rates in patients with CRC remains unclear, highlighting the need for further comprehensive research.






留言 (0)