
記住我

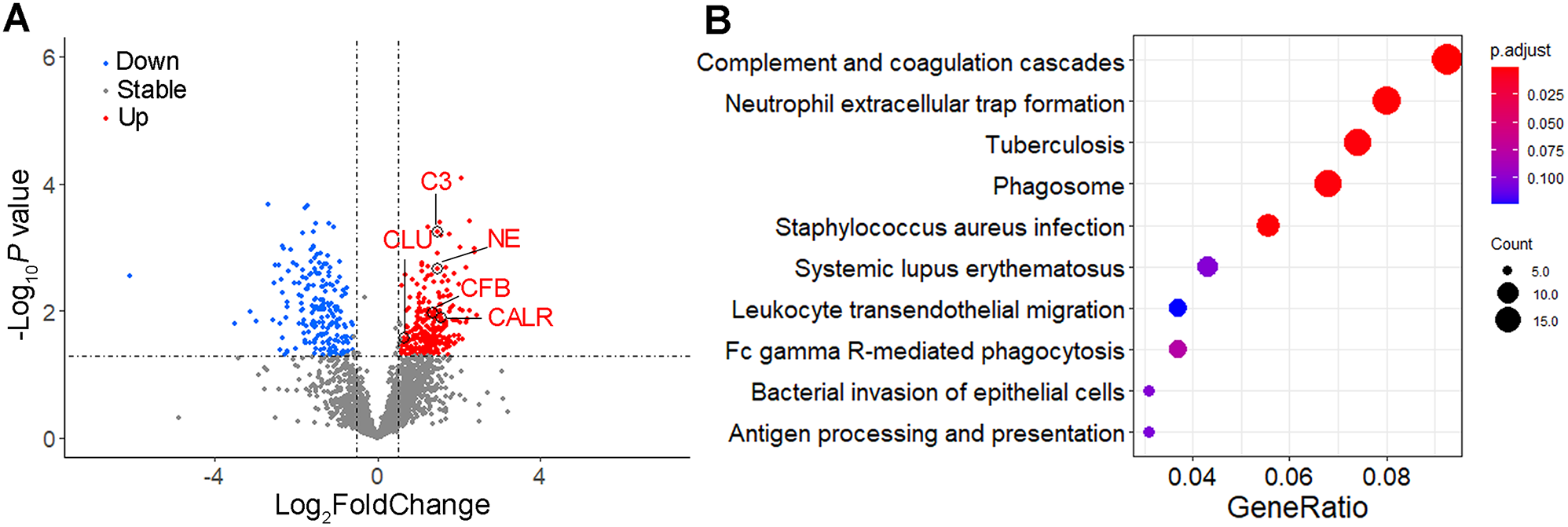



The proteins in saliva samples from patients with non-pSjD (n = 6) and pSjD (n = 6) were analyzed by mass spectrometry (Supplementary Table S1). 261 upregulated proteins and 198 downregulated proteins were found in the pSjD group compared to the non-pSjD group (Fig. 1A). To determine the functional roles associated with the upregulated proteins in the saliva of patients with pSjD, Kyoto Encyclopedia of Genes and Genomes (KEGG)-term analysis were performed. Complement and coagulation cascades, neutrophil extracellular trap formation, phagosome, and platelet activation pathways ranked high in the top ten categories (Fig. 1B).
Fig. 1
Differently expressed proteins in saliva of patients with pSjD compared to non-pSjD patients. (A) Volcano plot of differently expressed proteins in saliva of patients with pSjD compared to non-pSjD patients. Red indicates proteins with significantly increased expression in saliva of patients with pSjD. Blue indicates proteins with significantly decreased expression in saliva of patients with pSjD. (B) KEGG pathway enrichment bubble chart of significantly upregulated proteins in saliva of patients with pSjD
It is becoming increasingly evident that innate immunity plays a significant role in the pathogenesis of pSjD, particularly in autoimmunity initiation and progression [15]. Moreover, in glandular damage stage, complement activation is a result of humoral immunity which was considered as a dominant factor in pSjD pathology. According to the functional categories and earlier proteomic report [16], 5 upregulated proteins involved in innate immunity (C3, CFB, CLU, CALR, and NE) were selected for further experiments. Among them, C3, CFB, and CLU are components of complement cascades, NE participates in neutrophil extracellular trap formation, and CALR is involved in the phagosome pathway as well as a canonical type of damage-associated molecular patterns (DAMPs).
Comparison of the salivary biomarkers and clinical characteristics between pSjD and non-pSjD groupsA grand total of 186 patients were incorporated in the derivation cohort (Table 1). Among them, 121 patients (65%) were diagnosed as pSjD, and 65 patients (35%) were non-pSjD. To determine the difference of C3, CFB, CLU, CALR, and NE between the patients with pSjD and non-pSjD, we performed ELISA to quantify the concentration of these proteins in 186 saliva samples. The patients in the pSjD group had a notable increase in C3 (3784.00[1518.00-7192.00] ng/ml vs. 1551.00[829.00-3931.50] ng/ml, P < 0.001), CFB (489.85[255.55-923.03] ng/ml vs. 235.15[26.40-852.23] ng/ml, P = 0.001), CLU (517.45[289.13-1198.73] ng/ml vs. 135.60[50.20-293.50] ng/ml, P < 0.001), NE (95.54[0.00-247.21] ng/ml vs. 0.00[0.00-13.65] ng/ml, P < 0.001), and CALR (3.57[0.95–6.47] ng/ml vs. 2.24[0.93–4.14] ng/ml, P = 0.041) levels compared to those in the non-pSjD group (Fig. 2). The concentrations of C3, CFB, CLU, CALR, and NE of saliva samples from patients of rheumatoid arthritis (RA) or systemic lupus erythematosus (SLE) were also detected (Supplementary Fig. 1). However, C3, CFB, CLU, CALR, and NE levels from the RA or SLE group were slightly decreased without significant differences compared to the pSjD group. The data showed that these immune-related markers also presented in the saliva of patients with RA and SLE, suggesting limited value for classification between different systemic autoimmune diseases.
Table 1 Demographics and clinical characteristics of patient cohortFig. 2
The differences in levels of C3, CFB, CLU, CALR, and NE between pSjD and non-pSjD groups. The concentration of C3 (A), CFB (B), CLU (C), NE (D), and CALR (E) in saliva samples from pSjD (n = 121) and non-pSjD (n = 65) groups. Mann-Whitney U test was used to analyze data for differences Data are representative of 3 independent experiments. *, P < 0.05, **, P < 0.01, ***, P < 0.001, ****, P < 0.0001. pSjD, primary Sjögren’s disease; C3, Complement C3; CFB, Complement factor B; CLU, Clusterin; CALR, Calreticulin; NE, Neutrophil elastase
In addition to these 5 salivary proteins, there were 10 significantly different clinical characteristics between pSjD and non-pSjD groups, including uSFR, sSFR, Schirmer’s test, CRP, ESR, IgG, ANA titer, anti-SSA/Ro60, anti-SSA/Ro52, and anti-SSB/La (all P < 0.05). There were no differences between the groups in age, gender, RF, WBC count, serum C3 and C4 level (Table 1). To further validate the diagnostic power of C3, CFB, CLU, CALR, and NE to distinguish pSjD from non-pSjD, we performed ROC curve analysis. The area under curve (AUC) for C3 was 0.678 (95% CI 0.606–0.745), for CFB 0.631 (95% CI 0.558–0.701), for CLU 0.832 (95% CI 0.770–0.883), for NE 0.706 (95% CI 0.635–0.770), and for CALR 0.608 (95% CI 0.534–0.679), when used as single biomarkers (Fig. 3, Supplementary Table 2).
Fig. 3
ROC curve analysis of C3, CFB, CLU, CALR, and NE for distinguishing pSjD from non-pSjD. The ROC curves show the discrimination between pSjD and non-pSjD participants based on salivary C3, CFB, CLU, CALR, and NE. Area under the curve (AUC) for each ROC curve is shown in the figure. pSjD, primary Sjögren’s disease; C3, Complement C3; CFB, Complement factor B; CLU, Clusterin; CALR, Calreticulin; NE, Neutrophil elastase; AUC, area under the curve
3.3. Systemic disease activity and glandular function were compared between high- and low-level salivary protein groupsAccording to the ROC curve analysis and Youden index calculation, the optimal cut-off values to distinguish high and low levels of the salivary proteins were determined, at 2623.00 ng/ml for C3, 173.50 ng/ml for CFB, 221.40 ng/ml for CLU, 0.00 ng/ml for NE, and 3.78 ng/ml for CALR (Supplementary Table 2). To determine whether these salivary protein levels could reflect the systemic disease activity and exocrine glandular function, the 121 patients with pSjD were divided into the high-level group (> cut-off) and low-level group (≤ cut-off), and EULAR Sjögren’s Syndrome Disease Activity Index (ESSDAI) score, uSFR, sSFR, Schirmer’s test result, and focus score between them were compared. The C3-high, CFB-high, and CALR-high groups had significantly lower uSFR and sSFR than C3-low, CFB-low, and CALR-low groups, respectively, which suggested that these salivary proteins had the potential to reflect the secretory dysfunction of salivary gland (Fig. 4A-J). The levels of NE and CLU were not related to salivary flow. Similar ESSDAI scores, focus scores, and Schirmer’s test values were observed between groups of high- and low-level of these 5 salivary proteins (Fig. 4K-O, Supplementary Fig. 2).
Fig. 4
Comparisons of uSFR, sSFR, and ESSDAI score between high- and low-level salivary biomarker groups. The 121 pSjD patients were divided into high-level and low-level groups based on the cut-off value. uSFR, sSFR and ESSDAI score were compared between high- and low-level salivary biomarker groups. Mann-Whitney U test was used to analyze data for differences. Data are representative of 3 independent experiments. *, P < 0.05, **, P < 0.01, ***, P < 0.001, ****, P < 0.0001. C3, Complement C3; CFB, Complement factor B; CLU, Clusterin; NE, Neutrophil elastase; CALR, Calreticulin; uSFR, unstimulated salivary flow rate; sSFR, stimulated salivary flow rate; ESSDAI, EULAR Sjögren’s Syndrome Disease Activity Index
The combination of a non-invasive 6-biomarker (CFB, CLU, NE, anti-SSA/Ro60, anti-SSA/Ro52, and Schirmer’s test) model achieved significant discrimination of pSjDTo construct a non-invasive model for the diagnosis of pSjD, we utilize both univariate and multivariate logistic analysis. In the training cohort, univariate logistic regression analysis was conducted to examine the relationship between pSjD as a dependent variable while each salivary biomarker and clinical parameter as an independent variable (Supplementary Table 3). And there is no multicollinearity between the independent variables. Continuous variables such as C3, CFB, CLU, NE, and CALR levels were converted to categorical variables coded as 1 or 0 according to the cut-off level. uSFR and Schirmer’s test results were scored as either 1 (positive) or 0 (negative) according to the 2016 ACR/EULAR classification criteria. Categorical variables such as anti-SSA/Ro60, anti-SSA/Ro52, and anti-SSB/La were coded 0, 1, 2, and 3 according to the number of “+”. Both continuous and categorical values of C3, CFB, CLU, NE, CALR, uSFR, Schirmer’s test result, anti-SSA/Ro60, anti-SSA/Ro52, anti-SSB, ANA titer, ESR, and IgG were associated with a diagnosis of pSjD according to the univariate analysis (Supplementary Table 3). Multivariate analysis using a stepwise logistic regression model was performed to identify the final non-invasive predictors of pSjD. Candidate parameters of which P < 0.1 in univariate analysis were entered into the multivariate model. CFB, CLU, NE, anti-SSA/Ro60, anti-SSA/Ro52, and Schirmer’s test were retained in the non-invasive model as final variables (Supplementary Table 4). Hosmer-Lemeshow test revealed an adequate fit for the model studied (P = 0.402).
To determine the discriminatory ability of the combination of these 6 markers (CFB, CLU, NE, Schirmer’s test, anti-SSA/Ro60, anti-SSA/Ro52) for pSjD, the predicted probabilities (PRE) were calculated based on logistic regression analysis. For predicting pSjD, the following equation was used:
$$\eqalign} + 2.441 \times } + 1.237 \times } \cr & } + 1.194 \times }.} \times } \cr & }.} \times } \cr} $$
Based on the PRE of the logistic regression analysis, the AUC of the combined 6-marker model was 0.930 (P<0.001, 95% CI 0.877–0.965), with a sensitivity and specificity of 84.85% and 92.45%, respectively (Fig. 5A). Furthermore, this combined 6-marker model was able to better discriminate pSjD and non-pSjD, compared with each of the 6 variables retained in the model and the model containing anti-SSA/Ro60, anti-SSA/Ro52, and Schirmer’s test, the AUC of which was 0.832 (P < 0.001, 95% CI 0.767–0.896) (Supplementary Table 5, Fig. 5A).
Fig. 5
The diagnostic power of the combined 6-marker model for discovery and validation sets. ROC curves for the models including anti-SSA/Ro60, anti-SSA/Ro52, and Schirmer’s test alone (green lines) and with the inclusion of CFB, CLU, and NE (red lines) were shown (A-B). Discovery and validation cohorts were pooled together, ROC curves for the 6-marker models (red line) and MSGB alone (green line) were shown (C). ROC curves for the 6-marker models (red line) and model containing MSGB and Schirmer’s test (green line) were shown (D). The diagnostic power was assessed by calculating the AUC. ROC, receiver operating characteristic; AUC, area under the curve; CFB, Complement factor B; CLU, Clusterin; NE, Neutrophil elastase; MSGB, minor salivary gland biopsy
3.5. 6-marker Model validation in an independent setTo validate these findings further, we assessed the logistic regression model using a validation set consisting of 49 patients with pSjD and 23 patients with non-pSjD (Table 1). The resulting ROC curve had an AUC of 0.840 (P < 0.001, 95% CI 0.729–0.951), with a sensitivity and specificity of 78.72% and 86.36%, respectively. The model containing anti-SSA/Ro60, anti-SSA/Ro52, and Schirmer’s test had an AUC of 0.786 (P < 0.001, 95% CI 0.672-0.900) (Fig. 5B). Therefore, our study confirms the additional discriminatory value of salivary biomarkers in discriminating between patients with pSjD and non-pSjD.
To offer a non-invasive alternative to ease patients’ diagnosis, the diagnostic performance of the 6-marker model, minor salivary gland biopsy (MSGB), combined MSGB and Schirmer’s test was compared. Data from the discovery cohort and validation cohort were pooled for the analyses. The AUC of MSGB as a single variable to discriminate pSjD and non-pSjD was 0.793 (P < 0.001, 95% CI 0.753–0.833). The AUC for a model containing MSGB and Schirmer’s test was 0.870 (P < 0.001, 95% CI 0.828–0.911). The 6-marker model showed a better diagnostic performance than MSGB as a single variable, meanwhile achieving a comparable diagnostic value with the model containing MSGB and Schirmer’s test (Fig. 5C-D, Supplementary Table 6). These results suggested the 6-marker model could be a viable replacement for MGSB.
留言 (0)