Dermatochalasis (DC) is associated with eyelid skin elastic tissue loss and with impaired local lymphatic drainage [18]. Elastic fibers play an important structural and functional role in lymphatic drainage with clinical or subclinical inflammation leading to loss of elastic tissue and low- lymphatic output may well explain the phenomenon of “baggy” eyelids [19].
A significant familial, racial and ethnic anatomical differences exist in eyelid anatomy. "Double” and “single” eyelids, epicanthi and palpebral fissure slant, fuller or deeper sulcus, different composition of fatty tissue and variations of upper lid fold, making the distinction between different eyelids very important when taking surgical considerations [20].
Several techniques for treating DC are used including invasive and non – invasive treatments such as blepharoplasty and laser therapy [21]. Technique selection mainly depends on: the degree of DC surgical risk, preferences of the patient and experience of the operator [4].
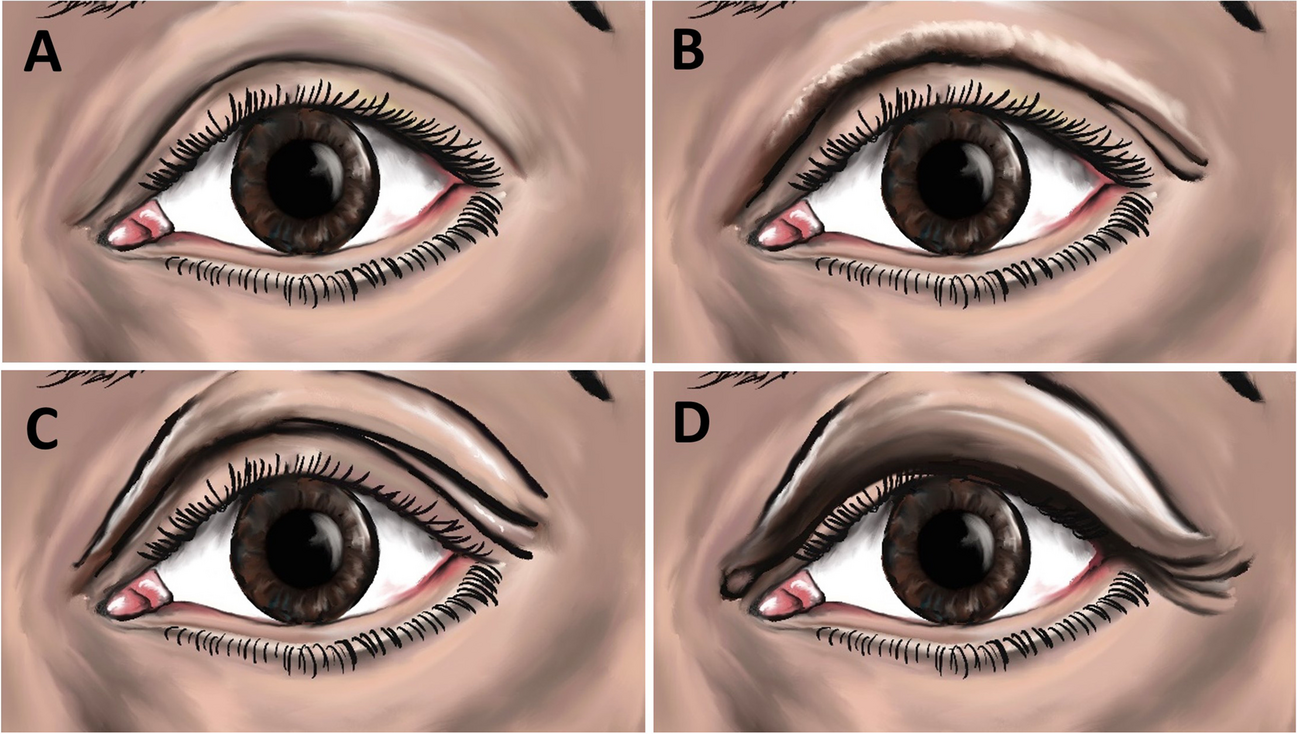
DC of the temporal region is well classified by the lateral DC classification [4]. This classification uses well-defined references of anatomical points, and may be assessed in frontal digital photographs, using horizontal lines as parameters to certify the correct anatomical points.
A pivotal feature of the blepharoplasty is its extension to the lateral region of the eyelid, until reaching the anatomical point three of the LDC, and the possibility of its association with other treatments, such as the suspension of the eyebrows and facial lifting [4].
Plasma skin regeneration is a novel type of skin rejuvenation technology [22] developed in recent years. The technology can present itself in four different phases: solid, liquid, gas, and plasma. By adding heat or energy to a gas, this is transformed into plasma: the atoms that make up the gas begin to lose their electrons and become positively charged ions. The lost electrons are then able to float freely and ionized. When this process involves most of the gas it is referred to as 'plasma' [23]. Devices using plasma technology deliver thermal energy directly to the tissues at the time of contact.
Hence, the two methods are different- surgery includes excision of the skin, some of the orbicularis muscle, and the prolapsed fat tissue. Plasma emesis is a non-invasive skin tightening procedure. Skin fibers contract and tighten, creating a lifting, remodeling, and rejuvenating effect. Plasma induces a denaturation of collagen and other proteins in the skin and follows a cascade of neo-collagenization, disruption of dermal solar elastosis, fibroblast activation and migration from the deeper dermis and cytokine release [17].
Previous studies have claimed that plasma radiofrequency ablation technology upper blepharoplasty could be recommended in mild and moderate DC without lipotosis [13, 14].
In this retrospective study we have found that in lateral DC plasma skin regeneration demonstrates good results in DC grade 0 to 1. Its' advantages include: no scaring, less tendency of hemorrhage, no incisions and stitches, shorter downtime, local anesthesia alone, no need for a whole surgical setting with lower patient costs, with yet desirable effects for the patient. However, from our experience in the following conditions non-satisfying results were demonstrated: lateral brow hooding, grade of excess skin is 2 or more, fat prolapse under the skin. In these conditions a surgical approach is likely to result in a better outcome, therefore patients who prefer a non-surgical approach should be set with realistic expectations, accordingly.
Naturally, these questions are addressed differently also according to the practitioner performing the treatment. A dermatologist would be prone to non-surgical solution, and the plastic or oculoplastic surgeon would likely tend to favor a surgical solution.
In our study we included two highly experienced esthetic physicians—one is dermatologist (LA), and the other in an oculoplastic surgeon (IAN).
Grading of dermatochalasis
For the purposes of the paper, we used the lateral dermatochalasis scales (LDC) classification of Silva etal [4] as it measures the main point of activation performed either surgically or by the plasma. Thus far, several scales have been developed to grade dermatochalasis of the upper eyelid [24,25,26].
The following are points to be taken into consideration for the decision of preferable method- surgical or non-surgical treatment.
The brow position
Brow ptosis is an important part of the preoperative assessment of blepharoplasty patients, especially when dealing with cases of lateral DC. When the brow descends, it compresses the soft tissues of the eyelid and weighs them down, often causing excess skin to prolapse over the lid margin and contact the eyelashes, a condition known as pseudoptosis.
When ptotic eyebrows accompany dermatochalasis, however, they often accentuate the upper eyelid abnormality and should be taken into consideration during surgery [27].
Patients with significant ptosis, heavy brows, medial greater than lateral ptosis, or post-facial palsy might not be good candidates for this procedure [28].
In such cases plasma treatment may be better, as it does not pull down the tissue. A subset of patients will manifest latent brow ptosis after eyelid surgery. It has been shown that ptosis surgery, whether done via Muller’s muscle conjunctival resection or by external levator advancement, leads to a decrease in brow height [29]. In cases of blepharoplasty alone, the change in brow height in studies are mixed [30]. Ptosis of the tail of the brow is the most frequently encountered brow deficit [31].
Eyebrows and eyelids vary among races, ages and genders. It is clear that each case is different and that adjusting the position of the eyelids and brows is complex, with interplay between muscles and connective tissue structures with neuronal pathways and interactions.
Safety
Safety of surgical solution are remarkably high, and complications are uncommon [12], however, there are possible complications mainly dry eye syndrome, corneal abrasion, cellulitis, asymmetry and scarring [32].
The safety of plasma exeresis in an animal model was previously demonstrated. Plasma has been shown to limit the damage within the connective parenchyma, enabling faster healing, both in the immediate and postoperative reparative processes as compared with electrosurgical/radio scalpel therapy [17].
Down time
For plasma exeresis one to three treatment sessions are needed at 2 months interval to achieve the optimal result. Patients should plan on 2–4 days down time and it takes about 12 weeks to see final results. In surgical blepharoplasty the healing process is significantly longer with bruising and edema around the eyelids. One can expect to spend approximately 2–3 weeks of resting and recovering.
Cost and Cover by insurance companies
Dermatochalasis is a unique condition as it is an aesthetic issue in its early stages and may develop later on to a medical indication for treatment. Eyelid surgery should improve abnormal function, reconstructs deformities, or enhances appearance and may be either reconstructive or cosmetic (aesthetic).
Blepharoplasty of the upper eyelids is considered reconstructive when it provides functional vision and/or visual field benefits or improves the functioning of a malformed or degenerated body member, but cosmetic when done to enhance aesthetic appearance. Medicare does not cover cosmetic surgery or expenses incurred in connection with such surgery [33]. In severe cases of DC, usually grade 3 in the measured stage we have used, Medicare would cover the surgery cost. In contrast, Plasma is never covered by the health insurance.



留言 (0)