
記住我





A 58-year-old man with a medical history of bariatric Roux-en‑Y gastric bypass (RYGB) surgery 9 years ago presented at our institution in 2021 with weight loss of 10 kg (body weight at the time of diagnosis: 129 kg), abdominal pain, diarrhea and hematochezia for the prior 2 months. Besides the gastric bypass, the patient had a history of idiopathic pulmonary embolism diagnosed in 2011. Regarding the family history, the patient reported that his father suffered from lung cancer.
Diagnostic workup included upper gastrointestinal (GI) endoscopy, which was unremarkable except for mild reflux esophagitis and colonoscopy, showing hemorrhoids grade 3 as potential cause of the bleeding. Due to persistent abdominal pain, we conducted an abdominal computed tomography (CT) scan with oral and intravenous contrast, which revealed para-aortic and mesenterial lymphadenopathy (Fig. 1). A thoracic CT scan demonstrated mediastinal lymphadenopathy. An endobronchial ultrasound-guided needle biopsy of paratracheal lymph nodes showed no evidence of malignancy. With persisting symptoms and extensive lymphadenopathy, we conducted an 18F-FDG PET-CT scan, detecting several cervical tracer-enriched lymph nodes and suspect lymph node stations in the mediastinum and abdomen. One suspicious, wire-marked supraclavicular lymph node was removed. Histological analysis demonstrated a poorly differentiated adenocarcinoma of gastrointestinal origin with HER2 positivity on FISH testing. Serum levels of CEA (18.3; normal 0–3 ng/mL) and CA72‑4 (11.1; normal 0–6.9 U/mL) were above the normal range. Although previous endoscopy showed normal findings, the histology strongly suggested a malignancy of gastrointestinal origin. Together with the department of nuclear medicine, we re-examined the diagnostic imaging, detecting slight tracer enrichment at the site of the gastric remnant. These results prompted an explorative laparoscopy to confirm the diagnosis. Wedge resection of the anterior wall of the gastric antrum was performed (Fig. 2). No peritoneal carcinosis or dissemination to other organs was detected. Subsequent histology taken from the gastric remnant confirmed the diagnosis of HER2-positive gastric cancer on immunohistochemistry testing (HER2 3+) with distant lymph node metastasis (intestinal type Lauren pT3, NX, L1, V1, R0, M1; UICC IV).
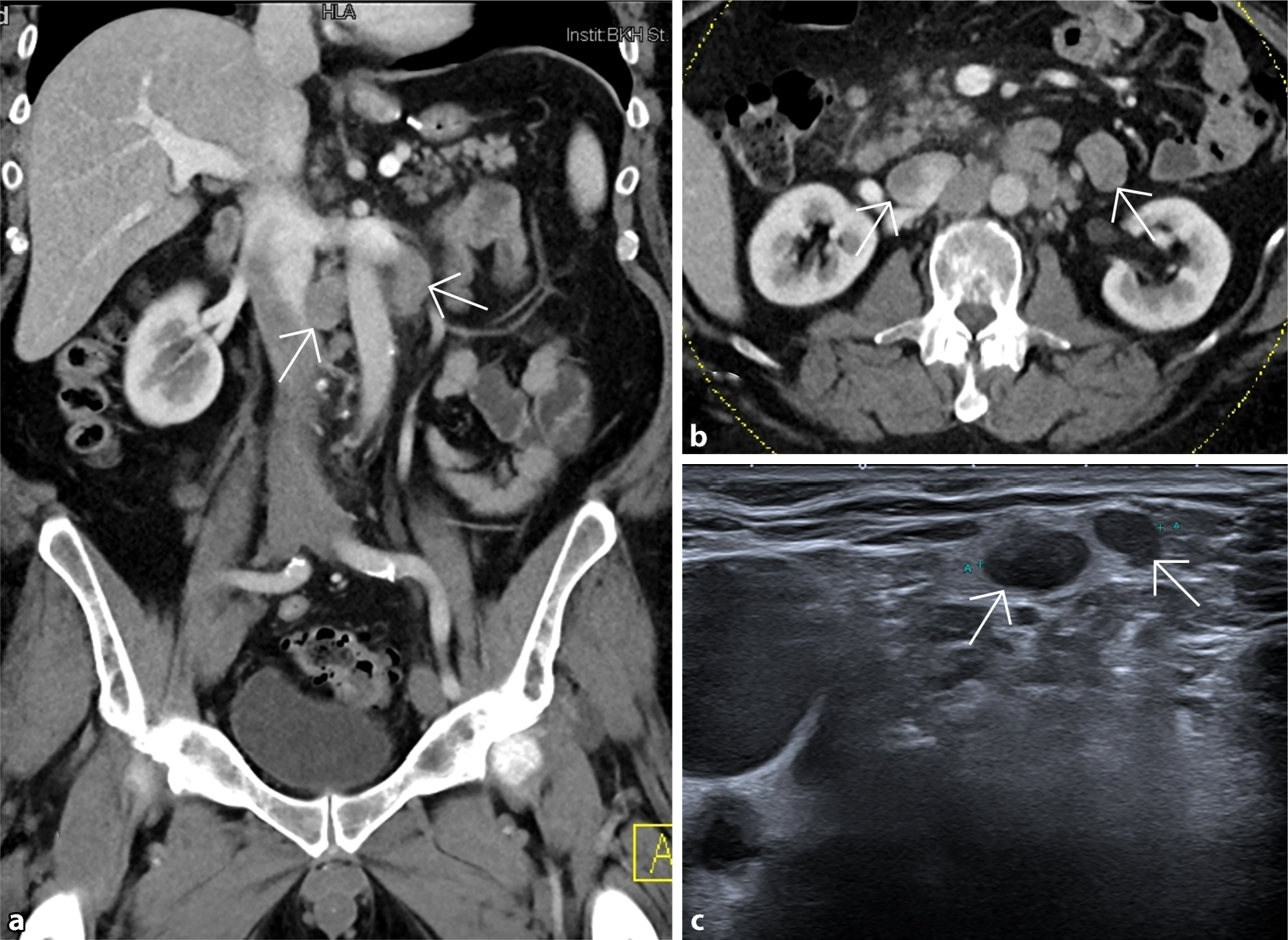
Fig. 1
a CT scan (frontal)—enlarged para-aortic lymph nodes, b CT scan (axial)—enlarged para-aortic lymph nodes, c ultrasound: 17 mm large wire-marked supraclavicular lymph node
Fig. 2
a Situation before wedge resection, b resected part: anterior wall of the gastric antrum, c situation following wedge resection
Our interdisciplinary tumor board discussed the treatment plan for this patient. We indicated a first-line therapy with trastuzumab, 5‑fluorouracil (5-FU), and oxaliplatin. Due to potential changes in the pharmacokinetics of orally administered 5‑FU after gastric resection, we chose intravenous administration using the FLO protocol in combination with trastuzumab (4 mg/kg) every 2 weeks, given the HER2 positivity. We excluded a DPD mutation before starting chemotherapy. After 7 cycles of FLO and trastuzumab, the patient’s tumor marker levels returned to normal. Restaging with PET-CT showed near-complete response. The patient developed grade 3 neuropathy as a side effect, prompting us to stop treatment. Maintenance therapy with trastuzumab was omitted in accordance with the patient’s wish to take a treatment break. Restaging with PET-CT 3 months after discontinuing therapy revealed progressive disease with lymphadenopathy and cholestasis, and a rise in tumor marker levels. The patient presented with painless jaundice due to malignant stenosis of the main bile duct and was transferred to a tertiary care hospital. Lumen-apposing metal stent (LAMS) gastrogastrostomy and endoscopic retrograde cholangiopancreatography (ERCP) were performed with stenting of the main bile duct. Unfortunately, the patient presented at our clinic shortly after this intervention with acute abdomen and sepsis. We presumed acute cholecystitis with a consecutive concealed perforation of the gallbladder as the cause in the CT scan. Therefore, we performed an emergency laparotomy showing an extensive peritonitis and biliary ascites due to a retroperitoneal leakage. Due to the findings after intra-abdominal lavage an abdominal-VAC was placed. Two days later a second look with conventional cholecystectomy was performed. We could not see any sign of gallbladder perforation, which is why, with the spontaneous cessation of the retroperitoneal leakage, a microperforation following ERCP was assumed. Apart from antibiotic therapy, no further intervention was necessary. The postoperative recovery was uneventful.
Therefore, a second line of chemotherapy treatment was commenced. There was no biopsy taken at the acute interventions but because of the previously known HER2 positivity we initiated treatment with trastuzumab deruxtecan through a named patient program. After three cycles, imaging and tumor levels showed partial remission, and the patient experienced no severe side effects. As of the last staging in October 2024, after 26 cycles, the disease remains stable.
留言 (0)