
記住我






In the IARC/WHO classification framework of neuroendocrine neoplasms (NENs), high-grade epithelial NENs refer to high-grade well-differentiated neuroendocrine tumors (NETs) (Grade 3 NETs; G3 NETs hereafter) and poorly differentiated neuroendocrine carcinomas (NECs). The distinction of G3 NETs from NECs has been regarded to be of clinical significance given their differing biologic behavior and response to therapies [1]. Intratumoral proliferative heterogeneity is a well-recognized feature of NENs. Moreover, Grade 1 (G1) and Grade 2 (G2) NETs may show progression towards G3 NETs. Although the possibility of NET-to-NEC progression sequence has been considered in the 2022 WHO classification of endocrine and neuroendocrine tumors [1], this requires further documentation.
Growing observations and recent publications have expanded the classification challenges related to a subset of G3 NETs due to their overlapping morphological features and/or acquired NEC-like molecular alterations during tumor progression, particularly in the context of multi-modal systemic therapies [2,3,4]. Backman et al. demonstrated that alkylating chemotherapy was associated with acquired mismatch repair deficiency (dMMR), DNA hypermutational phenotype (tumor mutational burden ≥ 50) and high-grade tumor progression in metastases originating from a subset of G1/G2 pancreatic NETs [2]. The authors suggested DNA damaging treatments may be contributing to tumor evolution, promoting mutagenesis and leading to high-grade transformation in some G1/G2 NETs [2].
In this issue of Endocrine Pathology, two important articles reported the correlates of progressive or lethal high-grade NENs originating from lower grade NETs. These articles advance our understanding of the biologic evolution of G3 NETs [3, 4].
Kasajima et al. reported acquired TP53 mutations and some NEC-like histological features (e.g., high-grade atypia, diffuse growth, necrosis) in a fraction of metastatic G3 NETs (7 pancreatic and 2 rectal G3 NETs out of 40 G3 NETs) that were associated with rapid tumor progression [3]. These metastatic G3 NETs all originated from NETs lacking NEC-like features, and had an initial median Ki67 labeling index of 10% (range: 3–28%) and a median Ki67 index of 65% (range: 50–85%) at the last examination during tumor progression. The authors named these biologically aggressive rapidly progressive high-grade NENs as NEC-like NETs. These tumors also retained common NET-related molecular alterations (e.g., MEN1, DAXX). Although more than half of these patients received alkylating chemotherapy as a component of their multimodal therapies, the microsatellite status was stable in all 9 tumors and only two had a tumor mutational burden ≥ 50. Despite the predominance of TP53 alterations, Kasajima et al. identified only one NEC-like NET acquired an RB1 alteration during disease progression [3].
In this issue, Joseph et al. also provided additional insight into the biologic and genetic evolution of rapidly progressive and lethal metastatic G3 NETs arising from lower grade NETs. Joseph et al. presented 5 patients with an initial G1/G2 or lower proliferative NET (3 pancreatic, 1 pituitary, and 1 unknown primary) [4]. In all 5 cases, RB1 and TP53 alterations were synchronously acquired in metastatic high-grade disease. These high-grade tumors also retained molecular alterations identified in the corresponding lower grade components. The Ki67 indices ranged between 60–94%. The reported median overall survival from the onset of high-grade transformation characterized by RB loss and aberrant p53 expression to the time of death was 12 months (range 4–41 months) [4].
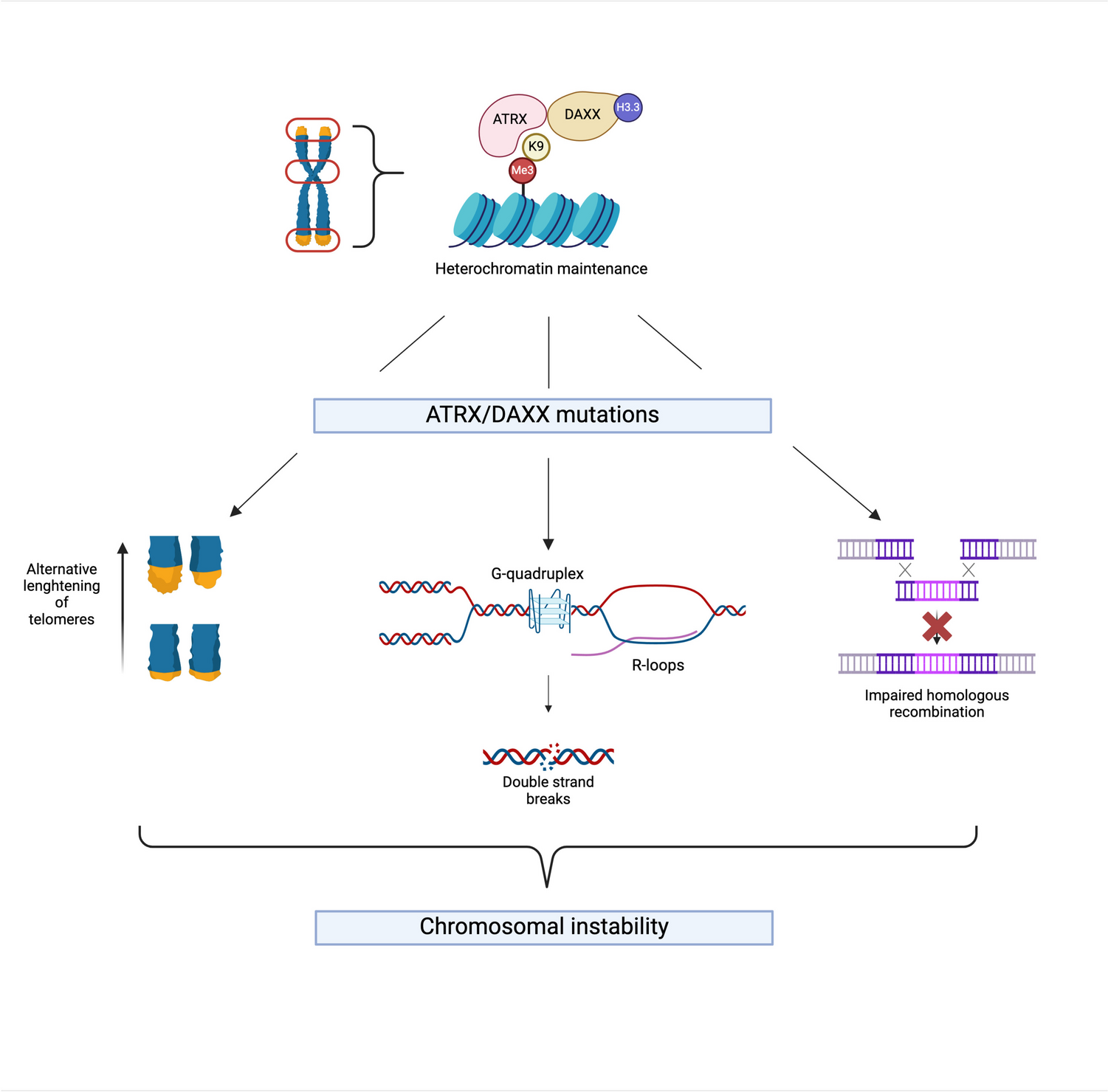
In contrast to various NETs, there is no formal WHO/IARC grading system in pituitary NENs. The correlates of high-grade disease are also largely undefined. Saeger et al. reported two examples of high-grade disease consisting of a G3 pituitary NET (G3 PitNET) and a presumed pituitary NEC (PitNEC) [5]. In this issue, Terry et al. reported a series of 13 patients manifesting with metastatic PitNETs, high-grade pituitary NENs and/or PitNET with sarcomatous transformation [6]. Eight patients died of disease, and all primary tumors had at least one adverse feature including aggressive tumor subtype, high-Ki67 indices and high-mitotic count. The median Ki67 index was 25% (range: 5–70%). ATRX deficiency was seen in one tumor, and p53 overexpression was seen in 3 specimens from 2 patients. TERT alterations were seen in three tumors among four tested tumors. While sarcomatous transformation cannot be justified as a form of NEC, the authors proposed the term of PitNET-ST for such occurrences. Although rare, the presented cases highlight the challenges in high-grade neoplasms.
Understanding the drivers of tumor progression is important for comprehending the biologic evolution of tumors. Evidence suggests that a subset of NETs can acquire TP53 and even RB1 alterations during their biologic evolution [3, 4]. Although the proper nomenclature for high-grade well-differentiated epithelial NENs that deviate from conventional G3 NETs (lacking TP53 and RB1 alterations and showing no NEC-like histological features) is yet to reach a consensus, evidence suggests the occurrence of NEC-like NETs, which represent the third biologically relevant category (Fig. 1).
Fig. 1
Acquired Biologic Evolution in Metastatic Spread of Neuroendocrine Tumors [2,3,4]. NET: Neuroendocrine tumor; NEC: Neuroendocrine carcinoma; TMB: Tumor Mutational Burden; dMMR: Mismatch Repair Deficiency; Increased Ki67: median 65% [3]
留言 (0)