Study population
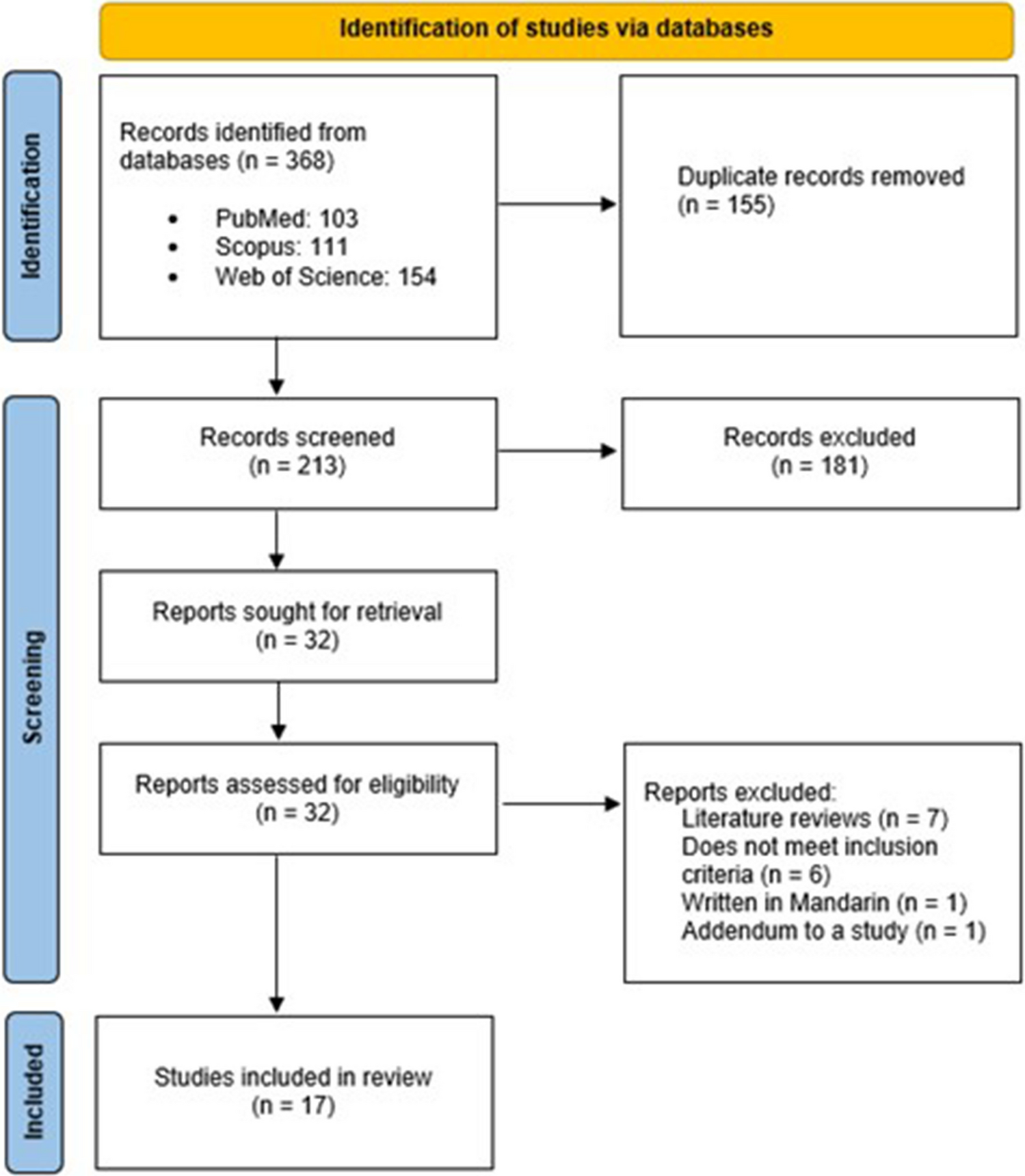
This was a population-based study using an online questionnaire to assess the symptom burden of post-COVID-19 conditions in children with a history of mild COVID-19 compared to those without a history of COVID-19. The questionnaire was distributed using Qualtrics, which is an online survey software program. Parents of children aged 4–18 years were invited by their schools to join this study and to fill in the questionnaire reporting their children’s post-COVID-19 symptoms and well-being. Meanwhile, adolescents and young adults between 12 and 24 years were also invited to fill in a self-report questionnaire reporting their post-COVID-19 symptoms and well-being. This study was approved by the ethics committee of the Institutional Review Board of the Hong Kong University/Hospital Authority Hong Kong West Cluster and Hospital Authority Central Institutional Review Board (Central IRB) (UW 20–292, UW 20–177, HKCH-REC-2022–009).
Between October 2022 and June 2023, the parent-report questionnaire was distributed to principals and parent groups at kindergartens, primary schools, and secondary schools in the five main districts in Hong Kong (Hong Kong Island, Kowloon East, Kowloon West, New Territories East, and New Territories West), while the self-report questionnaire was distributed to principals and parent groups at secondary schools and to the community. In Hong Kong, preschool children aged 3–6 years attend kindergarten. School-aged children aged 6 to 12 years attend primary school; adolescents aged 13 to 18 years attend secondary school. All parents and self-report participants were asked to give their informed consent and provide their demographic information. Potential duplicate entries or incomplete responders were removed. Children/adolescents outside the target age range were excluded from the analysis. Children with chronic illnesses or genetic disorders and children and adolescents with special educational needs (SEN) including physical disabilities, intellectual disabilities, visual impairment, hearing impairment, and psychiatric disorders were also excluded.
Development of the PCSS-C/Y
Based on the most prevalent symptoms highlighted in existing studies [6, 8, 13] and consensus from international bodies [4,5,6] and from a local expert panel (comprising of paediatric infectious disease expert, immunologist, neurologist, respirologist, cardiologist, developmental-behavioural paediatrician/rehabilitation specialist, general Post-COVID Symptom Scale for Children/Youth peadiatrician, neuropsychologist, child psychiatrist, and an ENT surgeon), we selected 17 post-COVID-19 symptoms most likely to cause impaired daily functioning in children and/or adolescents. These 17 symptoms were divided into four sub-domains and used as the basis for the development of PCSS-C/Y. The proposed PCSS-C/Y consisted of 17 items across four domains: (1) neurocognitive/brain fog symptoms (4 items), (2) cardiorespiratory symptoms (4 items), (3) olfactory symptoms (2 items), and (4) non-specific somatic symptoms (7 items). These items were scored on a 5-point Likert scale (0 = never to 4 = always). Participants with a history of mild COVID-19 (either self-reported or parent-reported) were asked to rate the frequency and severity of the symptoms lasting for at least 4 weeks since the initial phase of COVID-19 infection (7 days). Post-COVID Symptom Scale for Children/Youth (PCSS-C/Y) includes two forms: (1) a parent-report form for children aged 4 to 18 years, i.e. “Post-COVID Symptom Scale–Children (PCSS-C)” and (2) a self-report form for youth aged 12 to 24 years, i.e. “Post-COVID Symptom Scale–Youth (PCSS-Y)”. A sample question for PCSS-C was that “After your child has recovered from COVID-19 (starting seven days from the date of infection), please rate the extent to which the following persistent symptoms have affected your child. (Persistent symptoms are defined as those lasting for at least four weeks or more”. The non-infected control participants were asked to report their symptom severity in the last month. The items of PCSS-C/Y are listed in Table S1. The development process of the PCSS-C/Y is shown in supplementary file 2.
The originally developed PCSS-C/Y-20 had 20 items, but there were no significant differences between the post-COVID-19 participants and control participants in neuropsychiatric measures across all three sub-cohorts. As neuropsychiatric symptoms were not more frequently reported in post-COVID-19 cases compared to control subjects, the three items for neuropsychiatric symptoms were excluded from the current PCSS-C/Y scale. For the psychometric parameters of the original PCSS-C/Y-20, see supplementary file 3.
Other measurements
Health-related quality of life was assessed using the Paediatric Quality of Life Inventory (PedsQL) [14]. Children’s behavioural and emotional difficulties were assessed using the Strengths and Difficulties Questionnaire (SDQ) [15]. Demographic information, including family household income, where they lived, parents’ education level, and whether they were in receipt of social benefits, was obtained from the participants.
Scale construction and evaluation procedures
An exploratory factor analysis (EFA) was conducted to explore the factor structure of PCSS-C/Y and whether it aligns with the hypothesized symptom domains. As the scale was designed based on the four domains of symptoms, confirmatory factor analysis was performed to examine the factor loading structure of the proposed PCSS-C/Y. In this study, we used root-mean-square error of approximation (RMSEA), Tucker-Lewis Index (TLI), and Comparative Fit Index (CFI) to evaluate the factor structure, according to the guidelines by Hu and Bentler (1998) [16]. We considered an excellent fit as indicated by CFI ≥ 0.95, TLI ≥ 0.93, and RMSEA ≤ 0.06 and a good fit as indicated by CFI ≥ 0.90, TLI ≥ 0.88, and RMSEA ≤ 0.1. Reliability as a measure of internal consistency was assessed by Cronbach’s coefficient alpha. Correlational analyses were conducted to assess various indices of validity. The alpha level for statistical significance was set at 0.05. To interpret the significance of the correlations, we used Cohen’s (1988) criteria: r = 0.10 ~ 0.4 (small), 0.3 ~ 0.5 (moderate), > 0.5 (large).
Validity measuresKnown-group validity
Given that the prevalence of post-COVID-19 symptoms is small and that the severity of post-COVID-19 symptoms is reported to be mild, we envisage that the current scale can discriminate between the infected sample and control sample in terms of sub-domains and total post-COVID-19 symptom score with a Cohen’s d > 0.3.
Clinical validity
The clinical validity of PCSS-C/Y was determined by its correlation with PedsQL and SDQ. We recruited a sub-sample of participants to conduct a series of neurocognitive assessments including digital span task [17] and Conners’ continuous performance task [18]. We also administered an additional Sino-Nasal Outcome Test (SNOT-22) Questionnaire [19] to validate the olfactory sub-component of PCSS-C/Y.
Statistical method
Statistical analyses were performed using SPSS 28.0, SPSS AMOS, and R 4.1.0. Independent sample t-test was performed to assess discriminant validity, and a generalized linear model was used to evaluate the validity of PCSS-C/Y, with PCSS-C/Y or its sub-component inputted as the predictor, validation scales inputted as a criterion, and age and gender inputted as covariates. Partial R-square was used to evaluate the effect size of the correlation between PCSS-C/Y and the validation measurements.





留言 (0)