
記住我






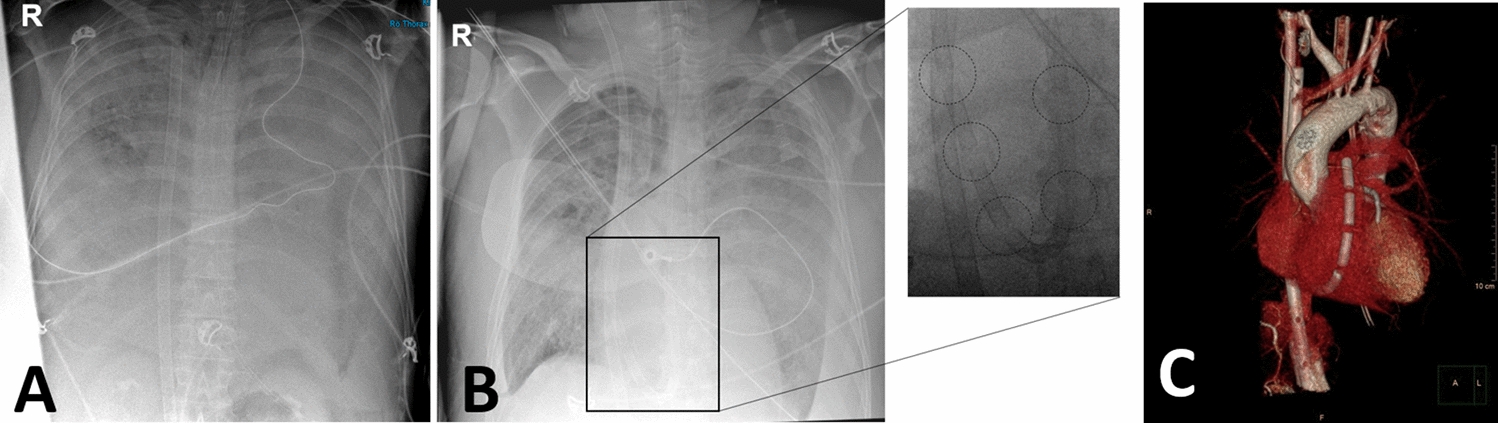
A 27-year-old patient suffered a penetrating thoracic injury from a knife attack and was transferred to our trauma center for specialized surgical and ICU treatment. At the time of admission, the patient was fully conscious and did not have motor deficits, respiration was compensated with two chest drains in place, but still a verifiable hemato-pneumothorax on chest radiograph (Fig. 1 Chest radiography upon ICU admission, with two indwelling left-sided chest drains in place, in the presence of persistent left sided pneumo- and hemothorax.); otherwise, the patient was in good and stable condition.
Fig. 1
Chest radiography upon ICU admission, with two indwelling left sided chest drains in place, in the presence of persistent left sided pneumo- and hemothorax
Three days after admission, the patient developed severe pneumonia and had to be intubated and ventilated. The remaining hematoma, not fully relieved by thoracic drains, was treated by video-assisted thoracoscopic surgery (VATS) the following day. Despite these interventions, as well as extended antibiotic coverage and adjunctive measures, the patient’s respiratory condition further deteriorated to severe acute respiratory distress syndrome (ARDS) and conservative treatment options were exhausted. Therefore, VV-ECMO (Maquet-Cardiohelp, Version 1, HLS Set Advanced 7.0; 23 Fr. V. jugularis interna (Inflow), 25 Fr. V. femoralis sinistra (Outflow)) was initiated as a rescue measure according to criteria established in the EOLIA-trial (PaO2/FIO2 < 50 mmHg at FIO2 ≥ 80% for > 3 h despite the optimization of ventilation and the duration of mechanical ventilation ≤ 6 days) [5]. The initial settings included a pump flow of 5 L/min and a sweep-gas flow of 10 L/min. Tracheostomy had already been performed.
The further course was complicated by an infected wound, remaining hematoma, and pneumatocele, all of which had to be surgically treated while still on ECMO. After 31 days of ECMO and ICU treatment, lung function had recovered so that spontaneous breathing could be established after reduction in sedation while still on VV-ECMO. When sedation was reduced, the patient gradually became conscious, however, due to severe critical illness acquired weakness syndrome, ventilation/carbon dioxide removal remained problematic for a prolonged period of time, while oxygenation was almost unimpaired [22]. Consequently, circuit blood flow could be reduced to 2.5–3.5 L/min, while the sweep-gas flow had to be remained between 2 and 4 L/min initially. Under these conditions, a protocolized gradual reduction in sweep-gas flow to 0 L/min was introduced to begin the final ECMO weaning step. However, due to an anxious patient, despite increased sedation, including the use of dexmedetomidine, adequate calming could not be achieved and the usual parameters to detect ECMO weaning failure (SpO2 < 88%, patient distress, pronounced tachypnea, pronounced tachycardia, and hypertension) were not conclusive. Due to our experience with NAVA during mechanical ventilation weaning, we attempted to use this mode during the final phase of ECMO weaning, that is, sweep-gas flow termination. The Edi peak was monitored and the ventilator settings were adapted throughout the weaning procedure. During NAVA-assisted weaning, we aimed to maintain the Edi peak generally within a range of 5–15 µV, with adjustments to the ventilator settings made if the Edi peak exceeded 15 µV. The Edi peak was used as a control parameter, and if it rose above 25 µV, despite ventilator adjustments, it was interpreted as diaphragm fatigue, leading to the immediate termination of the sweep-gas flow break as part of the individualized weaning protocol. Figure 2a shows an example of a ventilator graph during a sweep-gas flow of 6 L/min phase, with an Edi peak of 7.6 µV, and Fig. 2b shows the same patient during a phase of flow break phase with an Edi peak of 25.1 µV and the peak pressure terminated by the alarm setting immediately before the end of the sweep-gas flow break (Fig. 2 Ventilator graphics with NAVA a) before sweep-gas flow break b) after sweep-gas flow break). NAVA monitoring could effectively, conclusively, sooner than the usually used termination parameters, and independent of the patient’s fear, represent changes in diaphragm activation during sweep-gas flow break. This is well illustrated in Table 1 with the essential ventilation parameters of an exemplary weaning process of a gas flow of 0 L/min between 06:00 and 08:30 (Table 1 Sweep gas flow break from 06:00 to 08:30).With this protocol, the sweep-gas flow-free time could be continuously extended and ECMO was successfully removed on day 27 after admission without significant complications (Fig. 3).
Fig. 2
Chest radiography following ECMO and Tracheostomy tube placement in ARDS
Table 1 Sweep-gas flow break from 06:00 to 08:30Fig. 3
a before gas flow break b after gas flow break
The further weaning from mechanical ventilation went quickly and smoothly, all wounds healed by and by and were finally surgically covered. The patient was discharged 49 days after admission to a rehabilitation facility with mild swallowing difficulties and critical illness myopathy and polyneuropathy. The tracheostomy was covered with dressings and no abnormalities in gas exchange were observed without oxygen supply.
留言 (0)