
記住我





In total, 13 value sets have been published for EU-27 countries, 31% in the Western European region (according to the United Nations Statistics Division (UNSD)), 23% in the Northern European region, Southern European region and Eastern European region – Table 1. Most (85%) used EQ-VT protocol versions 2.0 and 2.1, while only the Netherlands and Spain (15%) used version 1.0. Year of publication ranged from 2016 to 2023. 54% of studies used stratified sampling. Regarding elicitation techniques, 77% of studies used a hybrid final model, combining both cTTO and DCE data. Some studies (15%) used a Censored Tobit model with TTO data only, while others opted for different models. The number of respondents varied, with some falling below the recommended threshold of 1000 for deriving utilities from EQ-5D-5L [30].
Table 1 Summary information on included EQ-5D-5L study characteristics: country, UNSD sub-region, publication year, sampling method, sample size, protocol version, preference elicitation technique(s), value set model and ranking of relative importance of dimensions in each value setThe national value sets generally show globally similar relative importance of each dimension, with some country differences (Table 1). Symptomatic dimensions (PD and AD) were often identified as most important compared to functional ones (MO, UA, and SC). PD was most important in 9 countries (69%), AD in 3 countries (23%), and MO in 1 country (8%). UA was least important in 6 countries (46%), SC in 2 countries (15%), and MO in 1 country (8%). In 7 countries (54%), PD and AD were the top two dimensions, and in 8 countries (62%), the least important dimensions were from the functional group. Four countries (31%) had the exact same ranking: France, Portugal, Poland, and Romania. Analysing the value sets themselves, we found variation among coefficients for level 5 issues across the different dimensions, with Spain having the smallest value for UA (0.018) and Ireland the largest for AD (0.646). The coefficient value range also varied between countries, with Ireland having the largest range (0.65) and Spain the smallest (0.14).
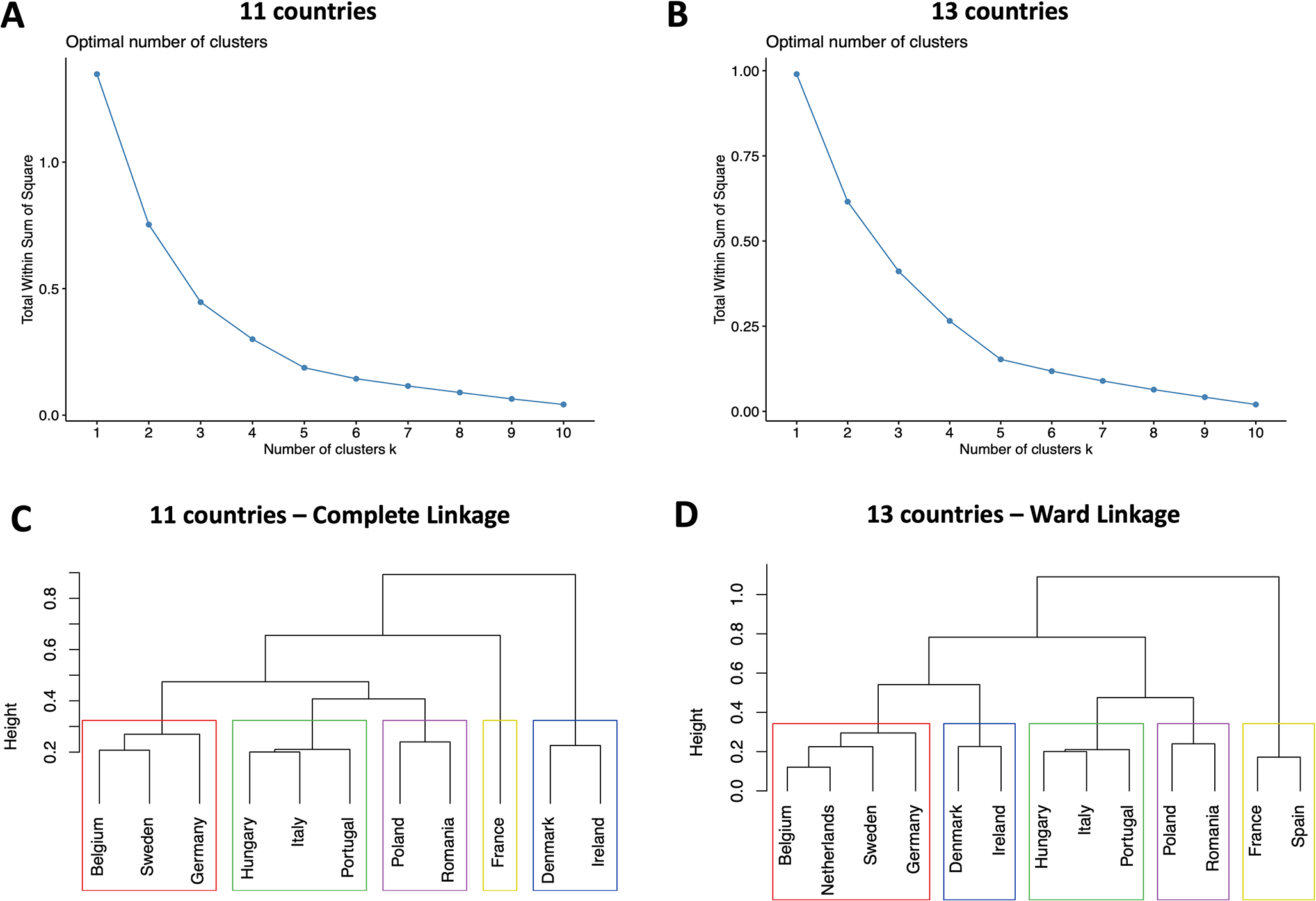
Cluster analysis of EQ-5D-5L value setsThe cluster analysis revealed strong structures using Ward linkage in the 13-country (AC = 0.813), and Complete linkage (AC = 0.706) in the 11-country analyses, with Elbow plots suggesting five clusters in both cases. Figure 1 shows the dendograms for these preferred cluster models and Elbow plots.
Fig. 1
Elbow evaluation method plots (A and B) and Dendograms (C and D) for the 11 and 13 country cluster analysis. Panel A: Elbow plot for the 11 country cluster analysis; Panel B: Elbow plot for the 13 country cluster analysis; Panel C: Dendogram for the 11 country cluster analysis; Panel D: Dendogram for the 13 country cluster analysis. NOTE: Coloured rectangles represent similar clusters across panels C and D
Results showed minimal differences between the 11 country analysis and 13 country analysis (the inclusion of the two countries (Spain and Netherlands) not using EQ protocols v2.0/2.1): Spain aligns with France in the 13 country analysis (Fig. 1 – panel D), and the Netherlands with Belgium, Sweden and Germany (Fig. 1 – panel D). In both analyses, the Dunn index was computed − 0.78 and 0.83 in the 13 and 11 country analyses, respectively, showing overall moderate to good quality clustering.
On the second stage, using simulated regression coefficients, Ward linkage is the preferred method in the 11 country (AC = 0.708) and 13 country analysis (AC = 0.749). Elbow plots again suggest an ideal number of 5 clusters. Figure 2 shows the dendograms for these preferred cluster models and respective Elbow plots.
Fig. 2
Elbow evaluation method plots (A and B) and Dendograms (C and D) for the 11 and 13 country cluster analysis (simulated). Panel A: Elbow plot for the 11 country cluster analysis; Panel B: Elbow plot for the 13 country cluster analysis; Panel C: Dendogram for the 11 country cluster analysis; Panel D: Dendogram for the 13 country cluster analysis. NOTE: Coloured rectangles represent the same clusters across panels C and D
Again, results from the 11 country analysis and 13 country analysis are only slightly different: Fig. 2 – panels C and D). However, the inclusion of these two countries now produced changes in the green cluster, which took in Romania; Poland is alone in the purple cluster in both cases (Fig. 2 – panels C and D). The Dunn index was computed once again − 0.59 and 0.22 in the 13 and 11 country analyses, respectively, showing worse quality clustering than the non-simulated analyses.
Globally, there are no large differences between the non-simulated (Fig. 1) and simulated (Fig. 2) cluster analyses. Belgium, Sweden, Germany and the Netherlands are consistently in the red cluster; Hungary, Italy and Portugal in the green cluster, and Denmark and Ireland in the blue cluster. The purple and, particularly, the yellow clusters were the ones with the largest variations, which suggests these clusters may be absorbing value sets that are less similar between them than the other clusters, making them less well-balanced groups. Taking into account that the non-simulated analyses showed better values for the Dunn Index and the strongest clustering structure (through the AC) was found for the 13 country cluster analysis with the regression coefficients, this is our preferred cluster structure and main estimation.
There is variation in the relative importance of dimensions for each cluster considering both single-dimension level 3 and level 5 issues – Table 2. Considering single-dimension level 5 issues, symptomatic dimensions (PD and AD) are typically rated highest: PD was the most important dimension in all clusters except the blue, which prioritized AD. While PD and AD were the two most important dimensions in the blue and red clusters, PD was followed by MO in the remaining three clusters. UA was the least important dimension in all clusters except the red. All clusters except the yellow (one of two that presented the most variation in country composition) presented the same dimension ranking in all performed analysis. When considering single-dimension level 3 issues the symptomatic dimensions are still the highest rated, but AD is generally more prioritized. AD was the most important dimension in the red, blue and green clusters (in the main analysis) and also in the yellow cluster (in the simulated analysis). UA was mostly considered the least important dimension, as in the level 5 profile, but the ranking of the other dimensions was somewhat different at this severity level. Indeed, while MO was usually the third most important dimension in the severity level 5 profile, in the level 3 profile it was much more commonly last or next to last. While AD was the most important dimension globally, the purple cluster was the only one that placed it last – and it was also the only cluster that placed it next to last in the severity level 5 profile. Finally, the blue cluster was the only one that showed the same dimension ranking in both profiles. This means that preferences generally varied with different severity levels: when considering the most extreme severity level, PD is the most highly valued dimension, while at a moderate severity level, AD takes the top spot, with some variability in the remaining dimensions.
Table 2 Relative importance of each dimension in each cluster, based on the comparison of values for health states with single-dimension level 5 issues (51111, 15111, 11511, 11151, 11115) and single-dimension level 3 issues (31111, 13111, 11311, 11131, 11113) across all countries, both in the 11 and 13 country analysesFigure 3 presents regression coefficients for levels in each dimension, relative to the reference level (severity level 1 = no problems) for all included value sets. Countries are grouped in clusters across all panels, according to our best cluster definition - results from the main estimation with 13 countries. Each panel represents one of the considered dimensions, and each dot is a country-dimension-level combination. Regression coefficients represent the decrement in health state valuation from moving from level 1 (perfect health) to levels 2 through 5 in each dimension. As expected, countries belonging to the same cluster present similar preferences for each severity dimension-level pair. Globally, PD and AD dimensions present the largest variation in health valuation across severity levels, and the UA dimension the least. All clusters except the yellow one show a clear gradient in health valuation decrement (as expected). However, the yellow cluster shows relatively stable coefficients across all severity levels and dimensions, with a similar trend from levels 2 through 4 in comparison to the other clusters and no further deterioration from level 4 to level 5, in stark contrast to the other clusters.The blue cluster presents the highest coefficients for AD, the green shows higher coefficients for MO, SC and UA.
These results show clear groups considering the value sets and regression coefficients across countries that could not be detected through a simple descriptive analysis or purely geographical divisions – reinforcing the importance of cluster analysis as our chosen method and validating our results.
Sensitivity analysis using K-means clustering yielded identical results – Online Resource 1.
Fig. 3
Dimension-level regression coefficient distribution in the included value sets, for each cluster in our main estimation (coefficient-based cluster analysis with 13 countries). Horizontal axis represents severity levels 2–5, relative to severity level 1 (no problems). Vertical axis represents coefficient values for each country (simple mean). Countries in the same cluster are represented by the same color and shape. Cluster 1 (Red) – Belgium, Netherlands, Sweden and Germany. Cluster 2 (Green) – Hungary, Italy and Portugal. Cluster 3 (Purple) - Poland and Romania. Cluster 4 (Yellow) – France and Spain. Cluster 5 (Blue) – Denmark and Ireland.
Legend: AD – Anxiety and Depression. MO – Mobility. PD – Pain and Discomfort. SC – Self-Care. UA – Usual Activities
留言 (0)