Patients
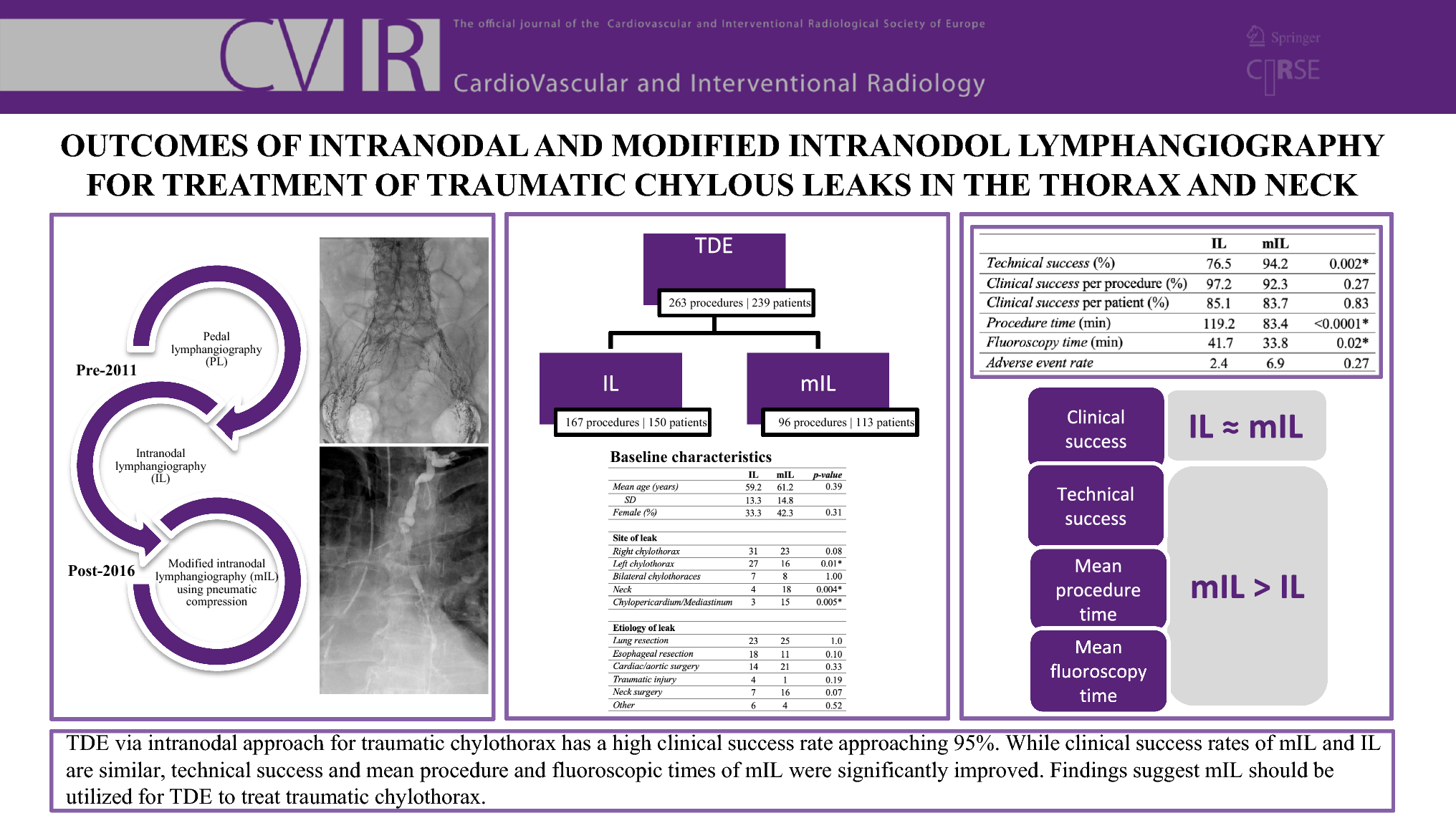
This study was approved by the institutional review board and is compliant with standards set forth by the Health Insurance Portability and Accountability Act. A retrospective review of a quality assurance database (Hi-IQ: ConexSys, Lincoln, RI) identifying all patients referred for TDE to treat refractory post-surgical chylous leaks in the thorax or neck at a single tertiary care center between 2002 and 2022 was performed. Patients who underwent a pedal approach to lymphangiography were excluded. All subjects who underwent intranodal lymphangiography for attempted TDE were included. All patients had chylothorax diagnosed by presence of white fluid from a chest tube or surgical drain with triglycerides > 150 mg/dL. Patients were categorized into IL (pre-2016) and modified IL (mIL, post-2016) cohorts. mIL incorporated the addition of pneumatic compression devices on the calves during and throughout lymphangiography and TDE. Baseline patient characteristics, including etiology and location of leak, are detailed in Table 1. The groups are not significantly different in age (p = 0.39), sex (p = 0.31), or etiology of chylous leak.
Table 1 Baseline characteristicsProcedures
The intranodal technique is described in detail below. All procedures were performed by board- and certificate of added qualification (CAQ)-certified attending physicians with 8–20 years’ experience. Major and minor adverse events were defined according to the Society of Interventional Radiology (IR) reporting standards [6].
Intranodal and Modified Intranodal Lymphangiography
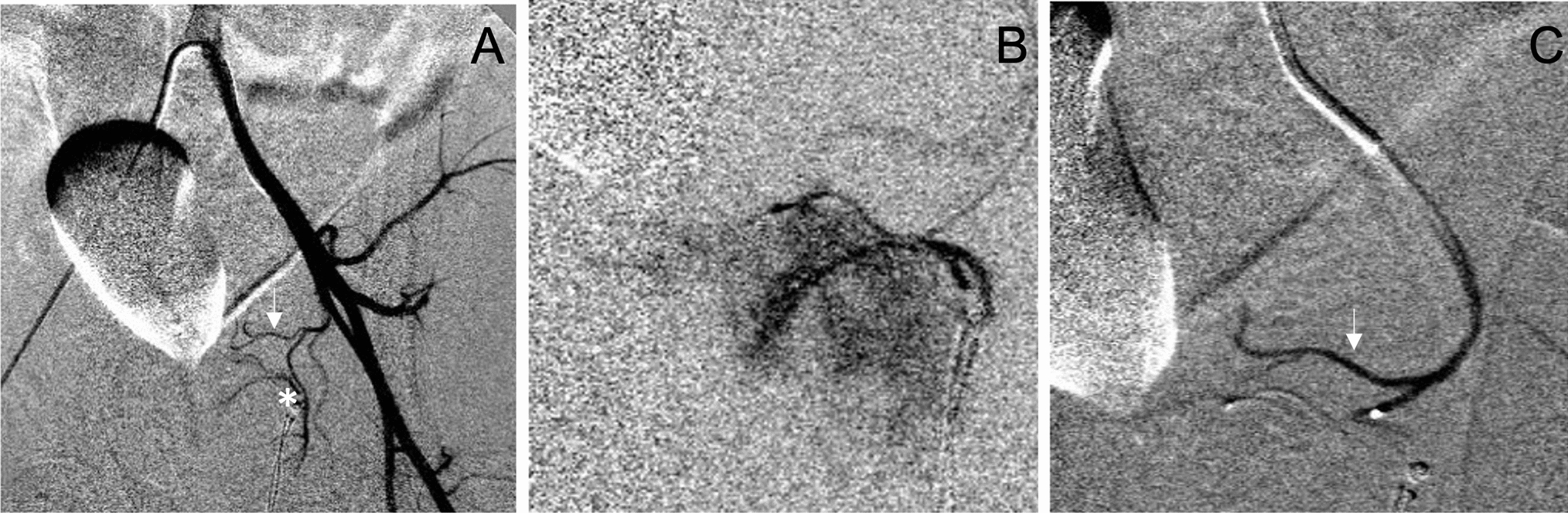
Using real-time ultrasound guidance, bilateral inguinal lymph nodes were accessed with the outer cannula of a 25-gauge spinal needle (BD, Franklin Lakes, NJ). The needle tip was positioned in the transitional zone between the cortex and hilum of the lymph node.
Under fluoroscopic guidance, ethiodol (Lipiodol, Guerbet, LLC Princeton, NJ) was injected by hand at a rate of about 0.1 mL per 1 min via short extension tubing and a 3 mL polycarbonate syringe (Merit Medical, South Jordan, UT). If an efferent lymphatic and/or lymph node was identified, further infusion of ethiodol was performed with a balloon insufflator preloaded with 10 mL of ethiodol. The insufflator was set to administer a pressure of 3 atmospheres to propagate the contrast into the lymphatic system. A total volume of approximately 6–12 mL of ethiodol was injected into each lymph node.
Infusion of ethiodol was terminated once lymphatics at the L3 level were opacified. If the cisterna chyli or upper abdominal lymphatics were not visualized at the end of the contrast injection, the initial bolus of ethiodol was followed by injection of normal saline at 1 mL per minute to facilitate propagation of the ethiodol. Since 2016, all patients undergoing intranodal lymphangiography utilized a modified intranodal technique (mIL) in which pneumatic sequential compression devices were placed on the bilateral calves during patient positioning. The pneumatic compression devices were activated prior to sterile preparation and draping of the patient to assist with lymphatic flow as previously described [5].
Thoracic Duct Cannulation and Embolization
Thoracic duct cannulation and embolization was performed as previously described [7]. Briefly, after the cisterna chyli and/or its contributing lymphatics were visualized with ethiodol, the lymphatic system below the cisterna chyli was accessed transabdominally under fluoroscopic guidance using a 21 or 22G Chiba needle. Using this access, a stiff 0.018″ wire (V-18, Boston Scientific, Natick, MA) was advanced into the TD followed by a 2.8F microcatheter (75 cm Rapid transit, Cordis Hialeah, FL or 100 cm Cantata, Cook Medical, Bloomington, IN). Nonionic iodinated contrast (Isovue-300) was then injected through the catheter to demonstrate the site of the chylous leak. Thoracic duct embolization was performed using a combination of platinum embolization coils (Nester, Cook Medical, Bloomington, IN) and N-butyl cyanoacrylate (N-BCA) glue (Truefill, Cordis Hialeah, FL) diluted with 1 mL of ethiodol.
Data Collection
Electronic medical records and imaging data were reviewed for demographic data, site/etiology of the chylous leak, procedure time, fluoroscopy time, technical success, clinical success, and adverse events. Procedure time was defined as the time from preoperative time-out to completion of the procedure. Preoperative time-out was obtained from electronic medical record documentation. Completion time was obtained from the final image documented during the procedure. Technical success was defined as successful cannulation of the cisterna chyli, regardless of clinical outcome. Clinical success was defined as the resolution of the chylous leak and removal of chest tubes or drains within 2 weeks of TDE, regardless of whether the cisterna chyli was cannulated or disrupted.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism 8.4.3 software (GraphPad Software, Inc.: San Diego, CA). A two-tailed Fisher’s exact test was used to compare baseline patient characteristics between groups and differences in technical success, clinical success, and adverse event rate. An unpaired two-tailed t test was used to compare differences in procedural and fluoroscopic times between groups. Descriptive data are presented as mean ± standard deviation. A p-value of < 0.05 was considered significant.


留言 (0)