Participants
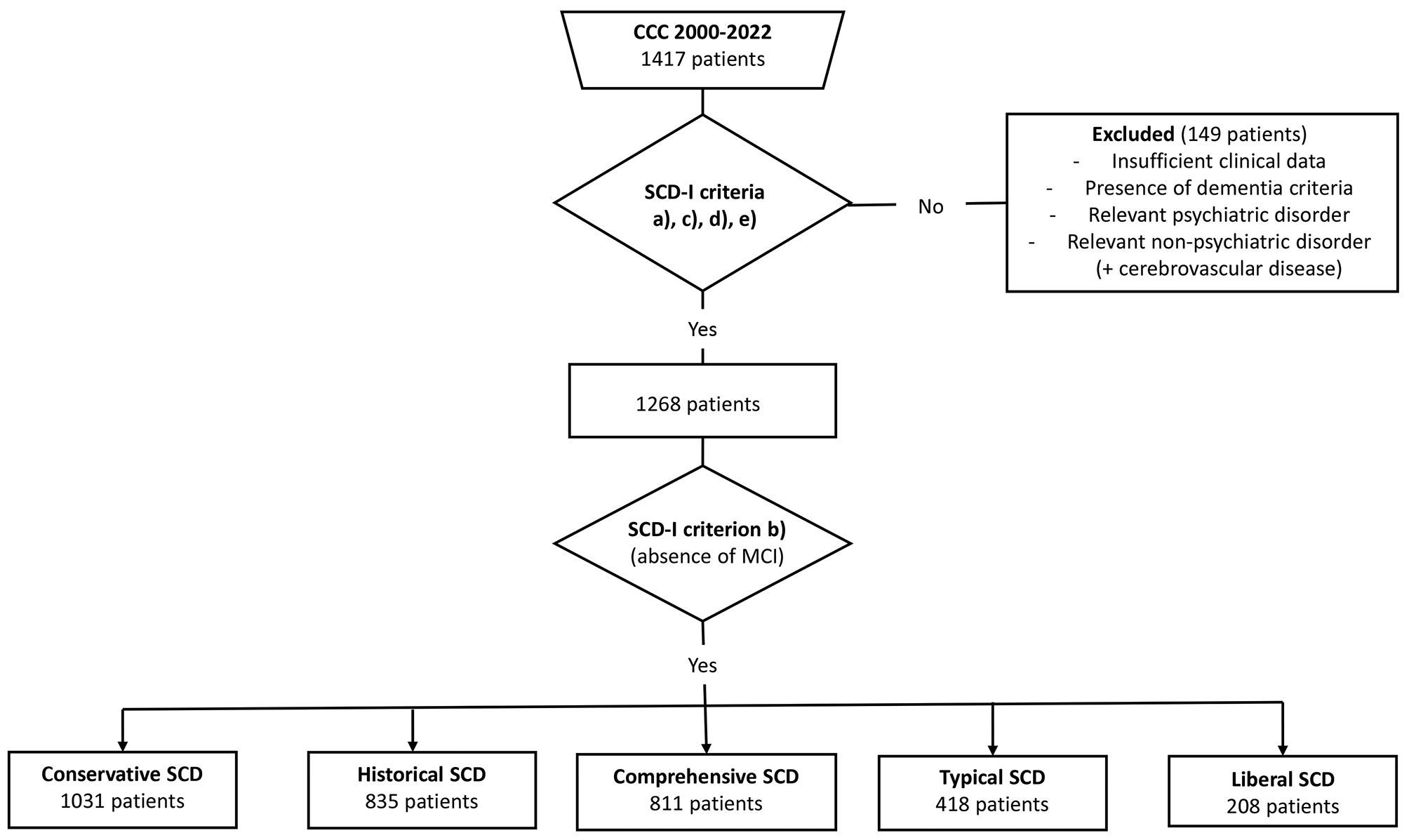
This study has a cross-sectional design, recruiting participants from the Cognitive Complaints Cohort (CCC). The CCC is a clinical cohort of non-demented patients with cognitive complaints established prospectively at the Faculty of Medicine, University of Lisbon [22]. The purpose of the CCC is to evaluate the outcome of subjects with cognitive complaints based on a comprehensive neuropsychological evaluation and other biomarkers. The same team of trained neuropsychologists performs the neuropsychological assessment at each CCC visit, following a standard protocol. The inclusion criteria of the CCC are (a) the presence of cognitive complaints and (b) having a detailed neuropsychological assessment. The exclusion criteria of the CCC are (a) the presence of neurological or psychiatric disorders that may induce cognitive deficits; patients with major depression according to Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR) [23] or serious depressive symptoms (indicated by a score of > 10 points on the Geriatric Depression Scale (GDS) short version [24]); (b) systemic illness with cerebral impact; (c) history of alcohol abuse or recurrent substance abuse or dependence and (d) presence of dementia according to DSM-IV-TR [23], or a Mini-Mental State Examination (MMSE) score below the cut-off for the Portuguese population [25], [26]. More detailed information concerning the establishment of the CCC has been previously published [27], [22], [28].
All the participants gave their informed consent to inclusion in the CCC. The study was conducted in accordance with the Declaration of Helsinki, and the local Ethics Committee of the Lisbon Academic Medical Centre (CAML) approved this specific study within the CCC. All the individuals included in the CCC between 2000 and 2022 were selected for the present study.
Diagnosis of SCD
The diagnosis of SCD was conducted by operationalizing the criteria proposed by SCD-I shown in Table 1 [13]: (a) Patients have self-experienced persistent decline if they presented to a memory clinic with a complaint of cognitive decline (SCD index criterion), and cognitive complaints were discriminated through clinical records and from the application of the Subjective Memory Complaints Scale (SMC scale) [29], [30]; (b) normal age and education-adjusted performance on extensive neuropsychological testing defined by the absence of MCI according to the five sets of MCI neuropsychologically based criteria defined by Jak and Bondi in 2009 [16] (Table 2); (c) normal global cognition defined in this study by a score ≥ 22 for those with 1–11 years of schooling and ≥ 27 for > 11 years on the MMSE [25], [26] and normal performance in activities of daily living defined in this study by a score < 3 on the first part (items 1–8) of the Blessed Dementia Rating Scale (BDRS) [31], [32], [33]; (d) absence of MCI according to the different MCI criteria examined by Jak et al. (2009) and used for criterion b) [16] or dementia defined according to DSM-IV-TR criteria [23]; (e) absence of past or present psychiatric or neurologic diseases, medical disorders, substance abuse, or use of medications that might explain the presence of subjective cognitive complaints. It should be noted that, regardless of the stage of clinical stability, patients with Neurodevelopmental Disorders, Schizophrenia Spectrum and Other Psychotic Disorders, Bipolar and Related Disorders, Depressive Disorders, and Obsessive-Compulsive and Related Disorders diagnoses according to DSM-IV-TR [23] criteria were excluded.
Table 2 Jak-Bondi MCI criteria [16]Significantly, the five different types of SCD considered will be determined by the Jak-Bondi rules chosen to define criterion b), as the remaining four criteria for the diagnosis of SCD remain unchanged. The SCD groups obtained by the absence of objective cognitive impairment were designated according to the respective Jak-Bondi criterion, for example, Historical SCD for the absence of Historical MCI, and so on.
The presence of SCD-plus variables (subjective decline in memory, rather than other domains of cognition, age at onset of SCD ≥ 60 years, onset of SCD within the last five years, confirmation of cognitive decline by an informant, concerns/worries associated with SCD, feeling of worse performance than others of the same age group and the presence of the APOE ε4 genotype), according to the research framework for SCD-I [13], was assessed through clinical records.
Sociodemographic data (age, sex, nationality, marital status, education, and profession), family history (psychiatric disorder and major or mild neurocognitive disorders), medical comorbidities (including the presence of arterial hypertension and diabetes mellitus), age at onset of the SCD, information regarding lifestyle, substance use, and usual medication were obtained through clinical records.
Subjective cognitive complaints
Data regarding subjective complaints were collected from clinical records, and the results of the SMC scale were applied to all patients included in CCC [29]. , [30] The SMC scale is a 10-item scale concerning difficulties in daily-life memory tasks, with total scores ranging from 0 (absence of complaints) to 21 (maximal complaints score).
Neuropsychological assessment
Global cognitive functioning data were collected from the results of the Portuguese version of the MMSE [25], [26]. The MMSE is a 30-point test, one of the most widely used brief instruments for clinical evaluation of cognitive state in adults.
Cognitive performance (age and education-adjusted) data were collected from the neuropsychological evaluation results using the Battery of Lisbon for the Assessment of Dementia (BLAD) [34], [35]. The BLAD is a comprehensive neuropsychological battery evaluating multiple cognitive domains, validated for the Portuguese population, that includes some tests from the Wechsler Memory Scale [36].
For this study, two tests from the BLAD, each with a missing data percentage below 10%, were chosen for the five cognitive domains identified by Jak and Bondi in 2009 [16]. The selected tests (domains) were logical memory delayed free recall, and five-word delayed free recall (memory); cancellation task and digit span forward (attention); verbal phonemic fluency and interpretation of proverbs (language); clock-drawing and Raven progressive matrices (visuospatial functioning); digit span backward and motor initiative (executive functioning) (Table 3).
Table 3 Neuropsychological testsData regarding performance in activities of daily living were collected from the results of the first part of the BDRS that addresses daily life activities [31], [32], [30]. The BDRS is a brief behavioral scale based on the interview of a close informant, assessing functional capacity for activities of daily living and changes in personality. This scale is composed of 22 items that address daily life activities (items 1–8), habits (items 9–11), and personality changes [12,13,14,15,16,17,18,19,20,21,22].
Neuropsychiatric symptoms
The GDS [30], [37] was used to characterize depressive symptoms. The GDS is a self-report assessment explicitly used to identify depression in the elderly. A short form (15 items) of the self-report instrument was used [24], [38]. Item 10 of the GDS, “Do you feel you have more problems with memory than most?” was treated as a distinct variable of interest since it does not dichotomously assess the presence or absence of memory complaints but rather seeks to evaluate their presence or absence using as a reference measure the memory complaints that most individuals would have. This aspect holds particular relevance, as research has demonstrated that variations in SCD measurement methodologies can influence the detection of early cognitive dysfunction [39]. , [40] The third part of BDRS evaluates personality and interests and drives changes. Clinical records were also reviewed for the presence of specific neuropsychiatric symptoms.
Statistical analysis
The statistical analyses, including multiple imputation, were performed using IBM SPSS Statistics for Windows, Version 28.0.1 (SPSS Inc., an IBM Company, Chicago, IL, USA).
An area-proportional Venn Diagram was generated to visually represent the differences and the similarities between the five SCD diagnostic groups using the DeepVenn Web application [41]. GraphPad Prism 10.2.0 (392) for Windows (GraphPad Software, Inc., San Diego, Calif., USA) was also used for graphical displays.
The sociodemographic, clinical, and neuropsychological data of each SCD diagnostic group were described using descriptive statistics. The neuropsychological assessments were standardized according to the age and education norms for the Portuguese population [42], and z-scores were calculated. The frequencies of SCD were computed considering the number of patients with SCD, according to the five different objective cognitive thresholds and considering three discrete intervals (0: absence of any SCD-plus variable; 1–3: presence of one to three SCD-plus variables, 4–7: presence of four or more SCD-plus variables).
To know whether the 5 SCD criteria might describe distinct patient populations, a bootstrap methodology [43] was employed to estimate the mean and 95% confidence intervals (CI) for specific parameters of interest, namely SMC scale (subjective cognitive complaints), MMSE (global cognition), BDRS first part (daily living functioning), and GDS (psychiatric symptoms), within each of the five SCD diagnostic groups. The means were considered statistically significantly different when the 95% CIs did not overlap (P2.5 and P97.5 were used as the limits of the non-parametric bootstrap CI for the mean).
Missing data were treated according to the principles of the TRIPOD statement [44]. Considering that the proportion of missing data among the ten employed neuropsychological tests was less than 10% and that the predominant absence of values in these variables is assumed to stem from random causes, the multiple imputation methodology [45], [46] was selected to address these variables. Recognizing the potential substantive contribution of additional variables to the imputed values, a multiple imputation model was formulated encompassing fourteen variables (ten neuropsychological tests, a metric for global cognitive performance (MMSE), a metric for subjective cognitive complaints (SMC scale), a metric for daily life functioning (first part of the BDRS), and a metric for neuropsychiatric symptoms (third part of the BDRS)). The automatic imputation method was selected in SPSS. After analyzing the data and considering that all fourteen variables were of a scale nature, SPSS employed the Monte Carlo method [47] for imputation, utilizing a linear regression analysis. Five sets of imputations were generated. The average of the five imputations for neuropsychological test variables was calculated to obtain the final data set.




留言 (0)