Study design and setting
A two-year prospective observational study was conducted at the AOU Careggi Multiple Pregnancy Outpatient Service in collaboration with the AOU Careggi Clinical Nutrition Unit, Florence, Italy, from October 2022 to May 2024. Twin-pregnant women enrolled during their initial obstetric visit underwent comprehensive monitoring throughout their pregnancy, with calorimetric, anthropometric, and dietary assessments conducted at three points: first trimester (8–13 weeks), second trimester (14–27 weeks), and third trimester (28–34 weeks). All participants underwent examinations between 7:30 am and 10:30 am following a 12-h fasting period.
The study received ethical approval from the Ethics Committee (CEAVC 21644/OSS, date of approval 13/07/2022) of the Tuscany Region, Careggi University Hospital, Florence. The study adhered to the principles outlined in the Declaration of Helsinki and the Data Protection Act. Informed consent was obtained from all participants.
Participants
Inclusion criteria comprised women aged ≥ 18 years with bichorionic biamniotic or monochorionic biamniotic twin pregnancies, whether spontaneous or obtained through assisted reproductive techniques. Exclusion criteria included age < 18 years, monochorionic monoamniotic or plurigeminal twin pregnancies, fetal genetic syndromes, metabolic conditions (e.g., pre-gestational diabetes mellitus), autoimmune diseases (e.g., dysthyroidism, systemic lupus erythematosus), psychiatric/eating disorders, malabsorption (e.g., chronic inflammatory bowel disease, coeliac disease), inability or unavailability to give informed consent, and/or non-understanding of the Italian language.
Data collection
Assessments and data collection were conducted at the AOU Careggi Multiple Pregnancy Outpatient Service and the Unit of Clinical Nutrition of the Careggi University Hospital by study staff. During the initial obstetric visit, participants were educated about the study's objectives and methods. Following their acceptance and signing of the informed consent, a nutritional visit was scheduled.
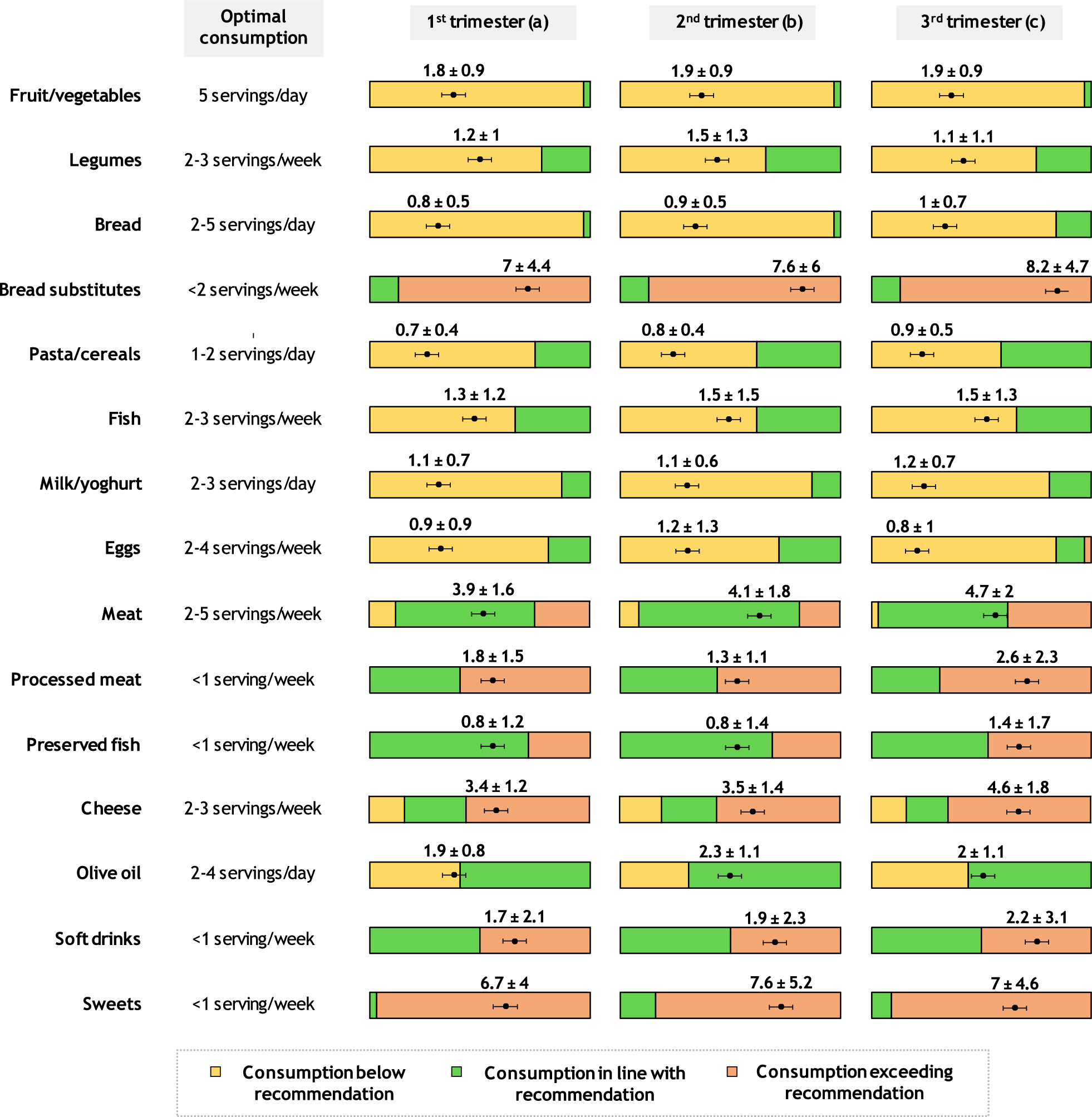
The standardized assessment included a questionnaire covering socio‐demographic variables, pre-pregnancy weight, body mass index (BMI), previous medical and obstetrical history, pharmacological therapy, family history, and risk factors. Participants were then asked to complete a weighted 7-day dietary record, detailing the type and quantity of food and drinks consumed at each meal. To assess the accuracy of reported intake, we evaluated each participant’s reported energy intake (EI) and used Goldberg’s EI:BMR cut-off values, as revised by Black [13, 14], to identify potential dietary misreporting. Based on this analysis, 12 women (38%) were classified as potential under-reporters. However, a nutritional consultation indicated that common pregnancy symptoms, such as nausea and gastric fullness, likely contributed to their reduced intake. Given our aim to assess actual intake while accounting for these side effects, we included all participants in the analysis. The Metadieta software (Me.Te.Da., San Benedetto del Tronto, Italy) was used to calculate the mean total daily intake of calories, macronutrients, micronutrients, and energy distribution for meals, and these values were compared to those recommended by the Society of Maternal–Fetal Medicine, which is generally accepted as a reference in twin pregnancy [15]. Additionally, the daily and weekly consumption of food groups and portion sizes were calculated based on the Italian Recommended Dietary Allowances (LARN) [16] and compared to the Italian Dietary Guidelines (CREA) [17]. Adherence to the Mediterranean diet was assessed using the Medi-Lite questionnaire [18], which assesses the consumption of nine food groups and categorizes consumption in accordance with the Mediterranean diet pattern. The final score ranges from 0 (low adherence) to 18 (high adherence).
Height and weight measurements were taken with a stadiometer and professional weighing scale, respectively, with BMI calculated as weight (kg)/height2 (m2). Ponderal status was defined using WHO standards for BMI cut-off points. The gestational weight gain (GWG) was compared to the Institute of Medicine (IOM) recommendations for twin pregnancy: 16.8–24.5 kg (37–54 lb) for women of normal weight, 14.1–22.7 kg (31–50 lb) for overweight women, and 11.3–19.1 kg (25–42 lb) for obese women [19].
Calorimetric assessment was conducted in fasting conditions using the Fitmate GS indirect calorimetry device (COSMED). The Fitmate GS is a portable desktop metabolic monitoring device that calculates resting metabolic rate (RMR), oxygen consumption (VO2), ventilatory power (VP), and expired fraction of oxygen (FEO2). Participants were instructed to fast for 12 h and avoid intense physical activity the day before the test. During the test, participants lay quietly for 30 min in a controlled environment, free from drafts, with a single operator present. After a 5-min calibration, VO2 was continuously measured for the next 25 min while participants remained awake but silent under a transparent hood. VO2 was averaged over this period and RMR was estimated using the abbreviated Weir equation: (3.9 × (VO2) + 1.1 × (RQ × VO2)) × 1.44, with a fixed RQ of 0.85. Additionally, RMR was estimated using the most commonly used predictive equations, as follows:
1.
Harris-Benedict Eq. (female): REE (kcal/day) = 655.1 + (9.56 × weight (kg)) + (1.85 × height (cm)) – (4.68 × age (years)) [20]
2.
Mifflin-St Jeor Eq. (female): REE (kcal/day) = (10 × weight (kg)) + (6.25 × height (cm))—(5 × age (years)) – 161 [21]
3.
Hronek Eq. (pregnancy): REE (kcal/day) = 346.44 + 13.96 × weight (kg) + 2.70 × height (cm)—6.83 × age (years) [22]
4.
Owen Eq. (female): REE (kcal/day) = 795 + 7,2 × weight (kg) [23]
5.
Schofield Eq. (female) [24]
age 18–30: REE (kcal/day) = 14.818 × weight (kg) + 486.6
age > 30: REE (kcal/day) = 8.126 × weight (kg) + 845.6
Hronek equation is the only one that was specifically validated for pregnant women with single foetus, while the others are referred to general female population.
Statistical analysis
Statistical analyses were performed using IBM Statistical Package for Social Science for Macintosh version 27.0 (SPSS 27.0; IBM Corp., Armonk, NY, USA) with a significance level set at p = 0.05. Categorical variables were presented as frequencies (percentages), while continuous variables were expressed as mean ± standard deviation (SD). One-way ANOVA models were employed for differences in continuous variables, and Chi-square tests for categorical variables. Pearson correlation coefficients were used for correlation analyses. A linear regression model for repeated measures was used to test changes in BMR across twin pregnancy. For this test, data were first normalized into logs and then, after data analysis, converted back to the original scale (antilog) to facilitate interpretation. Bland–Altman analysis and intraclass correlation coefficient (ICC) were used to assess agreement and reliability of predictive equations compared to indirect calorimetry in estimating BMR.

留言 (0)