Study aims
The present trial aimed to investigate the effect of IF on the body composition, health markers, and memory status among adults.
Study design
A multicentre, three-armed, parallel randomised controlled trial was conducted with an allocation ratio of 1:1:1 to examine the effectiveness of IF in improving the health indicators of overweight and obese, otherwise healthy adults. Participants’ blood pressure and anthropometric data (weight, BMI, and waist circumference) were the study’s primary endpoints. The secondary endpoints were fasting blood glucose levels and serum lipid profiles. The memory status of the participants was documented as a tertiary endpoint of the study.
Study setting
The present study was conducted in the Lahore district of Punjab, Pakistan. The study location was selected for its suitability for the participants, as statistics indicate a high prevalence of obesity and noncommunicable diseases among the district residents [18].
Participants and sample
People aged 40 to 60 years at the time of enlistment who agreed to participate and had a body mass index (BMI) > 25 were enrolled in the present trial from the corporate sector. This age limit was chosen because of the increased vulnerability to health issues related to short-term memory, blood pressure, blood sugar, and increased cholesterol levels [18, 19]. However, participants who were taking any statin medication, were terminally ill, had cancer, were pregnant or were taking anti-diabetic medicines were excluded from the present study.
A sample of 30 participants was calculated for each arm, with 80% power of the study, using 34.01 ± 6.48 as mean post HDL in control group and 38.62 ± 6.45 in intermittent group at 95% confidence interval (CI) using the formula given below [13].
$$}\,}\,}_}^}\,}\,}_2^}}\,}}_}}_}}_}}}}\,}\,}_}}}}^}}\} } \over }}_}}\,}\,}_}}}^}}}}$$
Trial groups and interventions
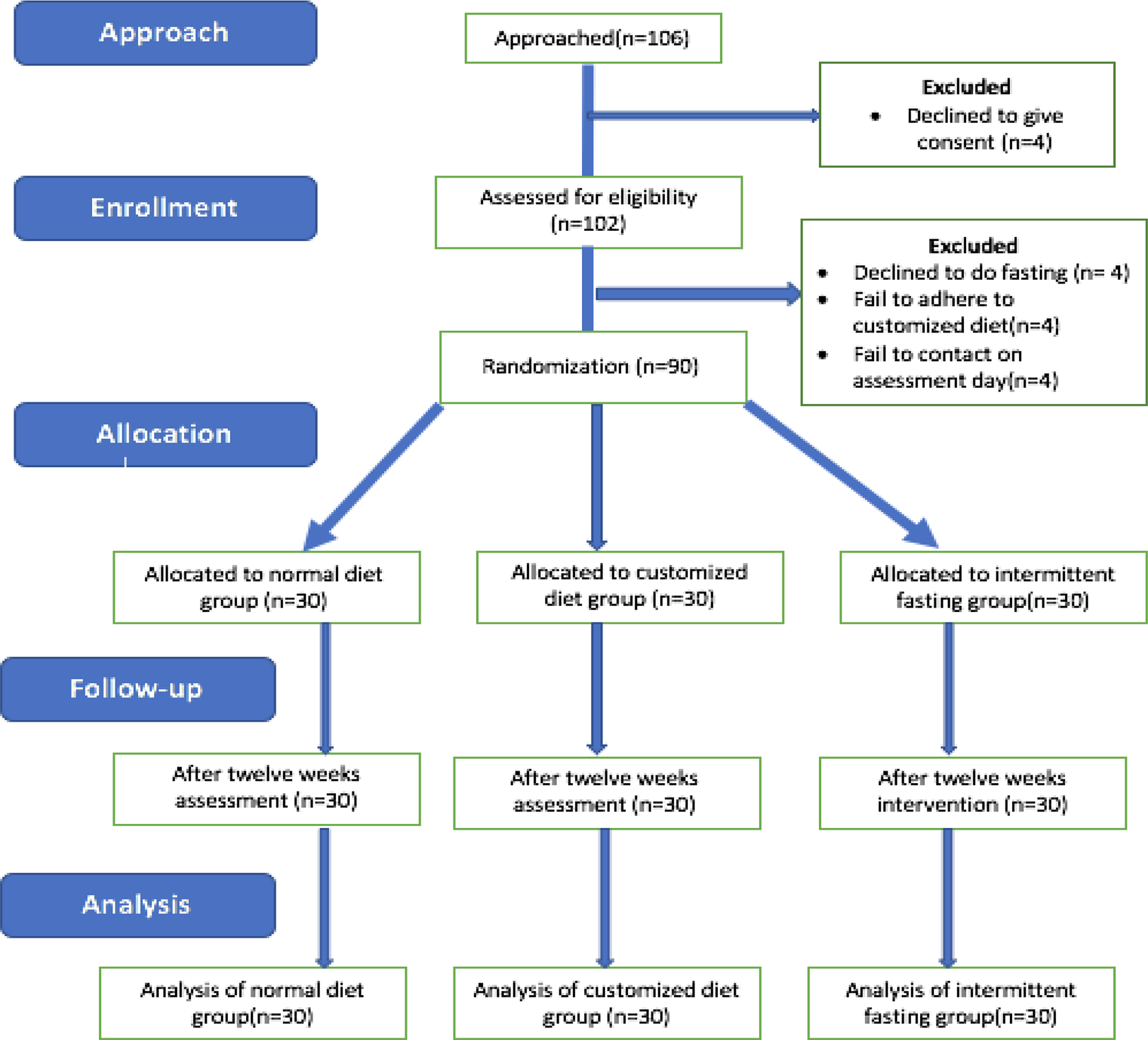
The participants were randomised into three groups, i.e., the control group, intervention group A and intervention group B. All the participants in the three groups were recruited for 12 weeks in the trial, and the following interventions were provided to each group.
Control group
No intervention was given to the participants recruited to the control group, and they were kept on a regular normal diet (ND). Members in the control group were encouraged not to change their eating regimen or their usual lifestyle during the trial period.
Intervention group A- IF
The participants recruited to intervention group A were kept on IF. The intervention IF group was given specific instructions to fast for approximately 16 h seven days a week, from 9 pm to 1 pm. They were urged to return to their regular dietary plan during 8 h of non-fasting intervals, i.e., 1 pm to 9 pm, with few instructions.
Specific instructions for the IF groupFasting period (16 h)
During the 16-hour fasting window, participants were advised to stay adequately hydrated with simple water, black coffee, black tea, or lemonade water with some fibre twice a day and to avoid carbonated and sugary beverages altogether.
Eating window (8 h)
During the 8 h of the eating window, participants were advised to break their 16-hour fast with a mixture of basil and chia seeds water, cumin water or honey and lime water. Furthermore, the participants were advised to use lentil soup and to replace simple carbohydrates with complex carbohydrates.
Intervention group B- customised diet (CD) plan
The participants recruited to intervention group B were kept on CD plans based on their BMI, which a certified dietician determined. For the CD group, after their BMI was taken and their caloric intake was assessed via 24-hour dietary recall, a simple CD primarily based on carbohydrate, protein and fat intake was prepared for them that could be quickly followed.
Randomisation and blinding
A statistician, independent of the study, created a random allocation sequence on a Microsoft Excel spreadsheet. Consecutive numbers were assigned to three arms. There were no restrictions (e.g., definition, block size). Two dietitians and one trained research nurse recruited participants and assigned them sequential ID numbers based on the grouping in which they were placed. The present trial was based on a single-blind methodology where only the investigator was blinded to the allocation.
Data collection and laboratory methods
At baseline, sociodemographic characteristics (age, sex, occupation) and physical activity were recorded using a structured questionnaire with a shortened version of the International Physical Activity Questionnaire (IPAQ) [20]. However, data related to anthropometric indices, blood parameters and memory status were collected at baseline and at the end of the trial. For anthropometric measurements and blood samples, participants were directed to the Government Teaching Hospital, i.e., Jinnah Hospital, where trained paramedic staff performed clinical assessments of participants at the hospital and recorded heart rate and blood pressure readings, both systolic and diastolic pressures, using a sphygmomanometer.
The staff captured the anthropometric data. BMI was calculated by dividing one’s height in meters squared by one’s weight in kilograms, while the participants’ wrist circumference was measured using a measuring tape when the participants exhaled normally, with the tape placed halfway between the iliac crest’s top and bottom edges.
The registered participants were then invited to a designated room in the Jinnah Hospital multidisciplinary laboratory. After each subject had fasted for 12 h, a skilled study nurse drew 5 ml blood samples by venipuncture. A Jinnah Hospital laboratory assistant collected blood to measure the serum cholesterol and blood glucose levels. The full-fasted lipid profile of each subject included total cholesterol, triglyceride, high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) levels. Serum lipid and fasting glucose (FBS) concentrations were estimated using a fully automated chemical immunoassay analyser (Abbott Alinity Ci analyzer). Standard laboratory techniques for assessing participants’ low- and high-density lipid profiles were used [21].
To capture individuals’ memory status, the Multifactorial Memory Questionnaire (MMQ) was used. The MMQ has three scales i.e., Satisfaction (a measure of worry about memory), Ability (a measure of subjective forgetfulness), and Strategy (a measure of compensatory memory strategies) consisting of 18–20 questions each, with a total of 57 items ranked on a 5-point Likert scale (1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = always) [22]. Improved satisfaction and ability are associated with higher scores on the MMQ subscales. Conversely, a lower score on the strategy scale aligns with the cognitive theory, suggesting that compensatory memory strategies involve techniques or modifications in behaviour or the environment to address deficits, weaknesses, injuries, or perceived inadequacies in a specific area or skill. A higher score on the strategy scale indicates a greater reported frequency of using memory aids and strategies compared to lower scores. The negative correlation between the strategy scale and Satisfaction and Ability implies that individuals with lower satisfaction and self-appraisal of memory are inclined to employ more memory strategies [23].
Follow-up and compliance
All the participants recruited from the three arms were followed for 12 weeks. Compliance was thoroughly monitored using a combination of weekly phone calls and messages throughout the trial duration. Participants were encouraged to visit the Jinnah Hospital outpatient department and given a dedicated contact number for a doctor or nutritionist in case of emergencies or any concerns. Treatment was free of charge for trial participants during the study period. After the follow-up of 12 weeks, anthropometric assessments and memory status assessments were performed by the study dietician and research nurse. A follow-up 5-mL blood sample was also taken from all participants who had completed the study for fasting blood sugar and serum cholesterol.
Ethical consideration and registration
The Departmental Doctoral Program Committee (DDPC) of the University of the Punjab, Lahore, approved the study (Letter No: D/119/ISCS), with the study registered at the registry of Clinicaltrials.gov with identity number NCT05521945. The present study was completed during a course of 1 year with the study registered on 30/08/22 and the follow-up of last participant completed on 11/08/23. The study was also carried out according to the Declaration of Helsinki.
Statistical analysis
IBM SPSS Statistics version 20 was used to analyse the data. The descriptive statistics of the qualitative variables are presented as the frequency (f) and percentage (%), while those of the quantitative variables are given as the mean standard deviation (SD) for normally distributed variables and the median ± interquartile range (IQR) for skewed variables. Furthermore, for inferential statistics, paired sample t-tests and Wilcoxon signed rank tests for normally distributed and skewed distributions, respectively, were used to assess the difference in the time component (pre- and post-comparison) for all three groups. For analysing the differences among groups (ND, CD and IF), analysis of variance (ANOVA) and the Kruskal‒Wallis test were applied. Finally, to analyse the differences in categorical variables among the three study groups, the chi-square test was applied. All the tests were applied at a 95% CI, with < 0.05 indicating statistical significance.




留言 (0)