
記住我


We conducted a retrospective cohort study using data from electronic medical records and follow-up visits. Typically, children were diagnosed with LGEA prenatally or within 1 month after birth and were then referred to the Department of Pediatric Surgery at Xinhua Hospital in Shanghai for treatment. Xinhua Hospital is a tertiary center serving patients nationwide, mainly from the Yangtze Delta region. Given that the reported incidence of LGEA was 1 per 40,000 live births [4], the nine cases of LGEA treated annually in Xinhua Hospital correspond to a population of about 0.36 million, significantly greater than the 0.07 million live births recorded in Shanghai in 2022 [16]. This study involved all children (n = 58) who underwent LGEA surgery at Xinhua Hospital between January 2016 and December 2023. The patients were scheduled for outpatient follow-ups after surgery three times before reaching three years of age: at 6 months, 12 months, and between 2 and 3 years of age. We excluded eight children who had only completed one follow-up because of missing data on the main outcome of long-term growth.
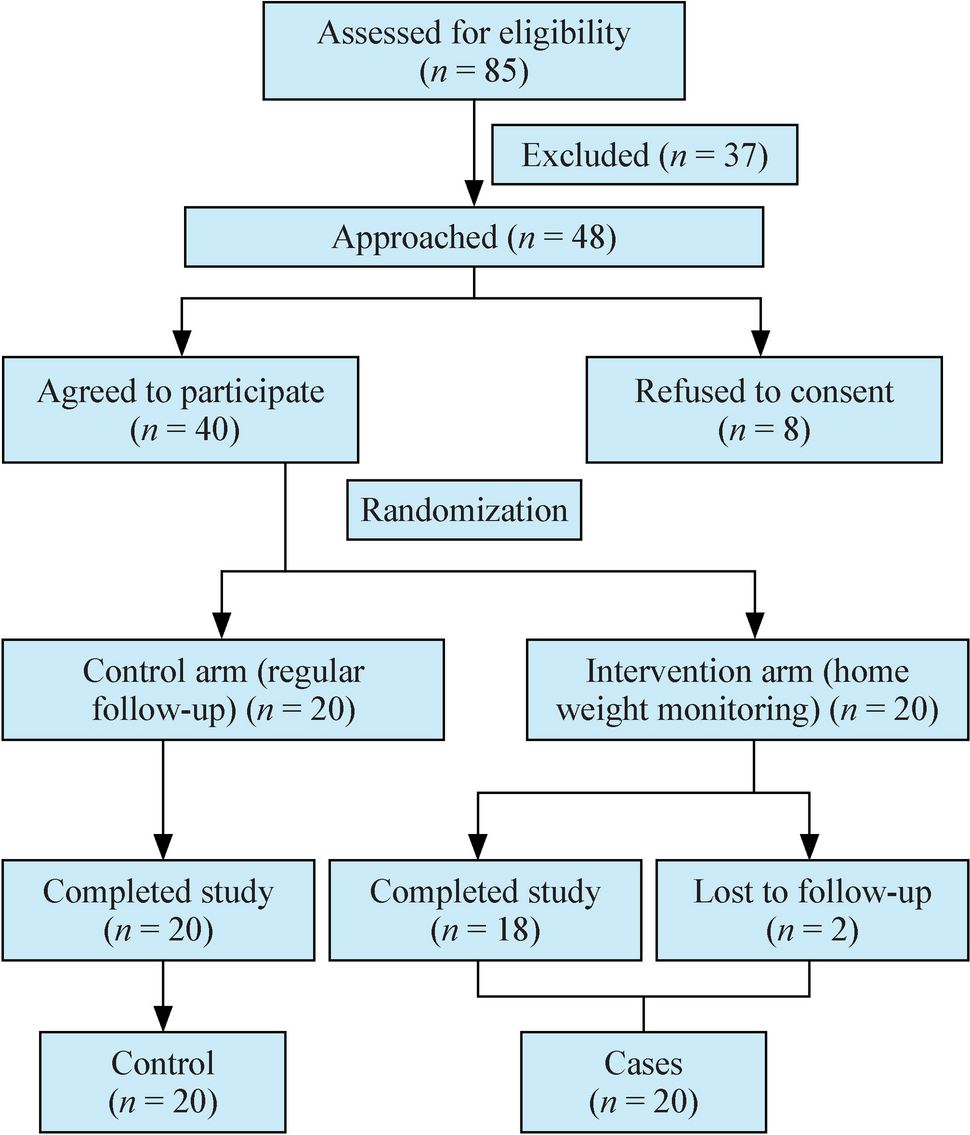
The majority of LGEA cases required a delayed primary anastomosis (see LGEA management below), which had been recognized to influence swallow function and associated with delayed oral feeding and growth outcomes. To improve the nutritional and growth outcomes of children who underwent LGEA surgery, a standardized CSE program was introduced in January 2020, in collaboration with the Department of Developmental and Behavioral Pediatrics. Traditionally, patients who experienced an extended duration before achieving full oral feeding were managed with expectant care within the surgical departments. Referrals to developmental pediatricians were typically reserved for cases where oral feeding was not established by 2–3 years of age, specifically when associated with certain conditions such as coughing while drinking water, a restricted diet limited to certain textures, or reliance on tube feeding. This practice continued until the implementation of the CSE program in 2020. Consequently, patients who underwent anastomosis before the introduction of the CSE program did not receive CSE and were thus included in the historical control group (n = 31). Conversely, patients who underwent anastomosis after the implementation of the CSE program received CSE and were included in the intervention group (n = 19).
LGEA assessment and managementEsophageal atresia was suspected based on prenatal imaging, which revealed a structure resembling a blind pouch-like shape in the upper esophagus, no stomach bubbles or a small stomach bubble, and a history of increased amniotic fluid after 24 weeks of pregnancy. Esophageal atresia was confirmed via a tube inserted in the baby’s nose or mouth cannot pass down into the stomach, and x-ray can confirm that the tube stops in the upper esophagus. Esophagography was performed to measure the distance between the proximal and distal segments of the esophagus. LGEA was defined as type I, type II, or type IIIa esophageal atresia with a distance between the two segments greater than 3 cm [4]. All patients diagnosed with LGEA underwent gastrostomy via a nutritional route, except for one patient who had a short distance from the blind pouch (3.5 cm) and underwent primary esophageal anastomosis. After gastrostomy, continuous suction in the upper pouch was applied to avoid aspiration pneumonia. A bougienage stretching technique was used in the hospital to shorten the gap between the proximal and distal segments of the esophagus [17]. Once satisfactory elongation was achieved, a tension-free anastomosis was performed via thoracoscopy in 48 of the 50 included children. For the two children whose elongation processes were unsatisfactory, esophageal replacement was performed to construct the esophagus (thoracotomy).
The management protocol for LGEA patients is depicted in Supplementary Fig. 1. The transition from fasting to full oral feeding involves a three-step process: parenteral and tube feeding, partial oral feeding, and full oral feeding. Briefly, after surgery, patients were required to fast until the anastomosis had healed, which was confirmed by esophageal radiography. The first esophageal radiography was arranged 7–10 days post-surgery, with subsequent radiographs conducted weekly if the anastomosis had not healed. Partial oral feeding was initiated once anastomosis healing was confirmed. Tube feeding was discontinued once full oral feeding could be achieved.
Clinical swallow evaluationsWe expanded this framework by integrating multiple pre-, peri-, and post-operative sessions, with each session comprising both evaluative and interventional components, tailored for patients with LGEA who underwent anastomosis (Supplementary Fig. 1). Briefly, a developmental–behavioral pediatrician (“the evaluator” WJL, Supplementary Table 3–5) conducted CSEs via individualized examinations and interventions during the pre-, peri- and post-surgery phases for LGEA patients. The objective was to develop age-appropriate eating skills and improve nutritional status. In this study, all CSE procedures were executed by one developmental-behavioral pediatrician (WJL) following an established protocol. First, the evaluator assessed the eating skills of each child to identify feeding problems that could delay the development of normal eating skills. This assessment included a preassessment case review, a caregiver interview, and a direct assessment. In the direct assessment, the evaluator examined the anatomy of the oral cavity, evaluated oral feeding mechanics including the functions of the lips, cheeks, tongue, and jaw, as well as related feeding proficiencies and assessed the coordination of feeding, swallowing, and breathing by administering 0.5–1 mL of water to infants using a syringe while simultaneously auscultating the neck [18]. Next, the evaluator screened for potential risk factors that could affect feeding difficulties, including swallow function, respiratory system, gastrointestinal/nutritional issues, the nervous system, developmental concerns, and other medical conditions. Then, the evaluator developed individualized therapeutic and feeding plans for patients. The therapeutic plan provided caregivers with advice on skill development and bedside instructions on relevant techniques. It further entailed administering targeted interventions aimed at fostering new skill acquisition, enhancing strength and coordination, and improving the safety of the swallowing process, such as the sequential introduction of liquids and solids, avoiding foods that did not align with the patient’s oral feeding capabilities, and food modifications to facilitate increased consumption. Individualized exercises such as simulated sucking, oral motor training, hand-to-mouth coordination activities, and non-nutritive bottle-sucking practice were also incorporated. Notably, the evaluator imparted essential exercises to the caregivers and offered individualized dietary advice, addressing aspects like food consistency and variety. This protocol guaranteed a regimen of daily practice sessions, occurring three to six times daily for optimal effectiveness.
CSE was systematically scheduled throughout the study’s duration, with a preoperative assessment conducted monthly. Postoperatively, CSE was administered a minimum of three to five times within the first postoperative year, initially at about 7–10 days post-anastomosis, with a subsequent evaluation at the one-month follow-up, and then evaluations every three months thereafter. For patients with esophageal dysfunction that limited their oral feeding capabilities, a re-evaluation was promptly arranged one week after the initial assessment to support the enhancement of the child’s feeding skills. If full oral feeding remained unattainable, monthly CSE re-evaluations were instituted to encourage further development in this area. When safe oral feeding was not feasible, oral exercise guidance was provided, followed by a reassessment three to seven days later, with weekly assessments continuing thereafter. During this period, the nursing team offered daily bedside intervention based on the assessment outcomes and instructed caregivers to facilitate three to six or more practice sessions daily. The protocol continued unchanged upon confirmation of the child’s safe oral feeding ability, with the frequency of evaluations primarily dictated by the developmental milestones of the child’s feeding skills. Patients in the treatment group received a minimum of one preoperative CSE and at least three postoperative CSEs. The evaluator delivered treatment and recommendations at the bedside during the patient’s hospital stay and continued this guidance during subsequent outpatient clinic visits. Notably, the recommendations focused on family empowerment through caregiver education, emphasizing that the intervention exercises were predominantly administered by caregivers both in the hospital and at home (Table 1).
The CSE program for LGEA patients was conducted in conjunction with various departments, including pediatric surgery, intensive care, nursing, pediatric respiratory, pediatric gastroenterology and nutrition, and otolaryngology departments. Referrals to pertinent specialties by the evaluator were made as required to support the patients’ comprehensive care. We present details of the CSE of one child who underwent LGEA surgery for a clearer understanding (Table 2, Fig. 1). The boy was diagnosed with congenital esophageal atresia (type I) through laparoscopic gastrostomy and distal esophagography. The distance between the two ends of the esophagus was 7.5 cm. After several rounds of pre- and postoperative CSE, the boy achieved full oral feeding at 8 months of age, 17 days after the anastomosis.
Table 2 A typical case of patient underwent clinical swallowing evaluation (CSE) programFig. 1
Typical clinical swallow evaluation interventions for a boy diagnosed with long-gap esophageal atresia. a before the operation, b during the perioperative period, and c during the postoperative period
Full oral feeding, physical measurement, and postoperative complicationsWe evaluated the feeding and growth status of the children after surgery using two primary outcomes: the period between surgery and full oral feeding, and the growth curve in early life. The time of full oral feeding was defined as the date on which a child demonstrated the ability to coordinate sucking, swallowing, and respiration for safe oral feeding, and tube feeding was discontinued [19]. Data on feeding conditions after surgery were collected weekly during hospitalization and every 3 months during outpatient follow-up. To analyze the period between surgery and full oral feeding, we defined a time-to-event period that started at the date of surgery and ended at the date of transition from tube feeding to full oral feeding, death, or loss to follow-up, whichever occurred first.
Length and weight data were collected through physical examination during outpatient follow-up. We calculated the length-for-age Z score (LAZ) and weight-for-age Z score (WAZ) using WHO Anthro software (version 3.2.2). We compared group-average growth curves for the WAZ and LAZ. These two growth curves fluctuate around zero for a normally developing child. In addition, we investigated stunting, defined as an LAZ < −2, and underweight, defined as a WAZ < −2, at 24 to 36 months of age [20, 21].
We recorded postoperative complications that occurred during hospitalization and outpatient follow-up, including pneumonia, anastomotic stenosis, reflux esophagitis, hiatal hernia, anastomotic leak, tracheo-esophageal fistula, and tracheal stenosis. All the data were extracted from electronic medical records and coded as yes or no during the follow-up period.
CovariablesWe selected potential confounders to establish the propensity score, including sex (male or female), age at surgery (in months), place of residence (urban, rural, or suburban), distance from the blind pouch of the esophagus before stretching (in cm), and weight at the time of surgery [19, 20]. We also included other clinical characteristics, including preterm birth status (yes or no), birth weight, prenatal diagnosis of LGEA, type of surgical procedure (thoracotomy or thoracoscopy), gastrostomy status (yes or no), and the presence of congenital anomalies (yes or no, for each type). Congenital anomalies included the following types: hypothyroidism, cleft palate, urinary system defects, cardiac malformations, skeletal muscle deformities, gastrointestinal malformations, and imperforate anus. All data were collected from electronic medical records.
Statistical analysisWe applied the inverse probability of treatment weighting (IPTW) approach to account for potential confounding factors. Briefly, a propensity score is the probability of a patient receiving the treatment of interest based on potential confounders (as described above). Logistic regression was applied to calculate the propensity score for each individual, using the ipwpoint function from the package ipw (version 1.2). Patients who received CSE were weighted by 1/propensity score and those who were in the reference group were weighted by 1/(1−propensity score). We used the standardized mean difference (SMD) to compare the differences in means (numerical variables) and proportions (categorical variables) of the baseline characteristics between the CSE group and the non-CSE group. Given the small sample size, an SMD < 0.2 was used as the threshold for an acceptable balance.
We performed all the analyses described below after IPTW. To investigate the association between CSE and the period between surgery and full oral feeding, we used the weighted Kaplan‒Meier method for visualization and the Cox proportional hazard model to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). In an additional analysis, we adjusted for the same set of covariates for comparison. Then, we used logistic regression to calculate the odds ratios (ORs) with corresponding 95% CIs for the associations between CSE and stunting at 2–3 years of age, underweight at 2–3 years of age, and postsurgical complications. Children without follow-up data between 2 and 3 years of age were not included in the investigation of stunting and underweight. Since there were no deaths during the follow-up period, we did not use methods considering competing events. We modeled the growth curves for WAZ and LAZ using a restricted cubic spline with three knots on age to account for potentially nonlinear growth patterns in the study period. All analyses were performed using R (version 4.2.1).
留言 (0)