
記住我

Study approval was obtained from an institutional review board. All patients had a signed written procedural informed consent, a study-specific informed consent was waived due to its retrospective nature. All patients who underwent MISACE procedure between May 2018 and July 2023 are evaluated, and the procedures with an angiographic-proven ASA have been included. Patient demographics as well as technical aspects such as puncture side, used catheters, relevant segmental artery to the ASA, maximal diameter of the aortic aneurysm, levels and numbers of occluded segmental arteries or any additional visceral branches, complications, and related follow-up data were assessed throughout the electronic patient recording system of our tertiary care center. The etiologies and the Crawford classification of the pathologies were analyzed [2].
MISACE ProcedureThe number and anatomy of the segmental arteries (SAs) relevant to preemptive embolization were evaluated using the patient’s preexisting CTA (computed tomography angiography) scans. The CTA protocol included an ECG-triggered arterial phase CT scan of the thoracoabdominal aorta, performed after the injection of 100 ml of intravenous contrast media. This was followed by 3D reconstructions of the acquired data (Fig. 1).
Fig. 1
CTA of the aorta. a Axial diameter of the aneurysm. b Sagittal reconstruction with an avid L-1 segmental artery c Coronal projection with a right Th-12 segmental artery. *CTA: computed tomography angiography, L: lumbal, Th: thoracal
After standart angiographic access through the groin, diagnostic catheters, such as Sim-I, C2, JR1, H1, and Special (Cook®, Angiodynamics®, Terumo®) were used to access the planned segmental arteries. A microcatheter of 2,4 F or 2,7 F of size (Progreat/Terumo®) with inner diameters of 0.021″ for MVP-3Q and 0.027″ for MVP-5Q, Medtronic®) was utilized to access the segmental arteries superselectively (Fig. 2).
Fig. 2
Schematic drawings. a of a microvascular plug (MVP), with the longer arrow pointing out the proximal marker, the short arrow being the distal marker. b Representation of a MVP placement in a segmental artery (SA: dotted black arrows) with a distally originated anterior spinal artery (ASA: curved black arrow) with the white arrow pointing the wire inside of a microcatheter with a placed but yet not permanently deployed MVP. *MVP: microvascular plug, SA: segmental artery, ASA: anterior spinal artery
Following the catheterization, the presence of the ASA was excluded with contrast injections, and the SA was occluded proximally with coils. The goal was to occlude up to four pairs of segmental arteries in a single session. If necessary, additional sessions were performed to complete the preemptive embolization.
MVP DeploymentOnce the anterior spinal artery-bearing segmental artery (ASAbSA) was angiographically suspected, it was carefully identified using focused and detailed angiograms. A microvascular plug (MVP) 3Q (for target vessels 1.5 to 3 mm) or 5Q (for target vessels 3 to 5 mm) was then precisely delivered through the microcatheter. After the intravenous administration of 5000 IU of heparin, the plug was carefully deployed in a very proximal position, with the aim of preserving retrograde perfusion to the ASA.
Before permanently detaching the device, we waited for 10 min with the MVP fully deployed but not yet released, in order to monitor for any immediate neurological side effects (e.g., paresthesia, paraparesis). This was done by continuously assessing the patient’s sensory responses and motor function, particularly in the feet. Once no adverse effects were observed, the MVP was permanently detached from its wire using a counterclockwise rotation (Fig. 3c).
Fig. 3
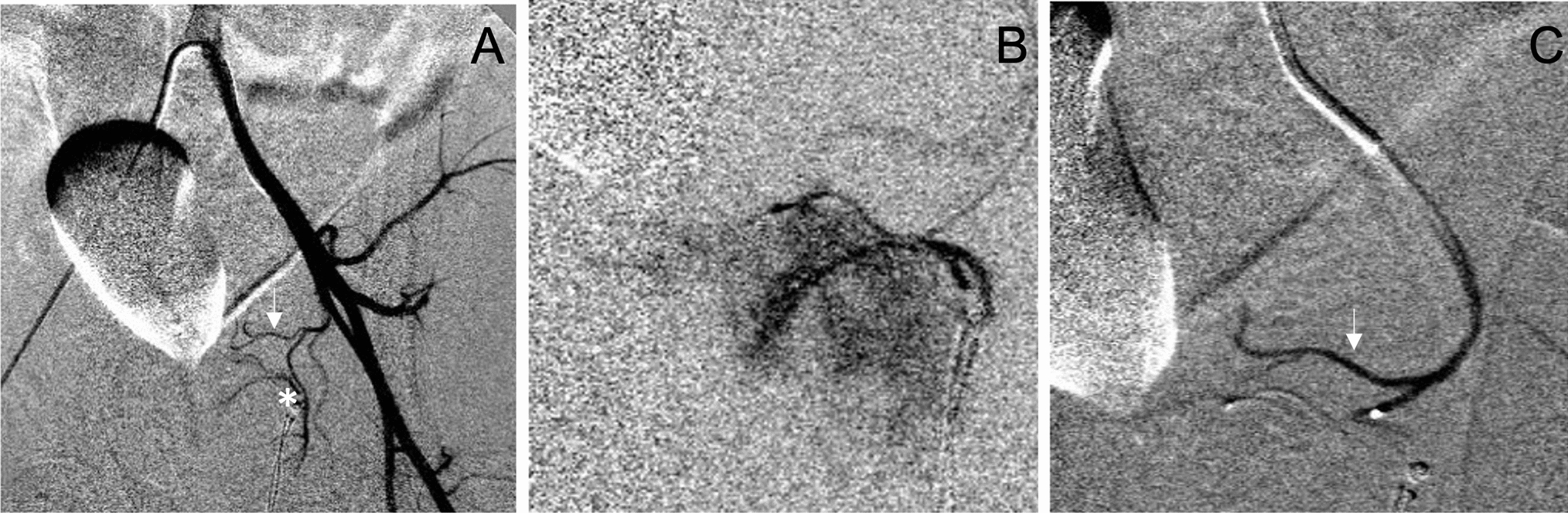
Stepwise deployment of the MVP at the anterior spinal artery bearing segmental artery (ASAbSA), proximal to the offspring of the ASA. a DSA of the L1-left lumbal artery feeding the anterior spinal artery (ASA, white solenoid arrow), straight white arrow pointing the offspring of the ASA. b Optional temporarily embolization with a proximally placed MVP-3Q Plug: Dotted white arrow shows the tip of the microcatheter, curved empty arrow points out the screw/detachment point of the plug. c Deployed plug at the proximal segmental artery (SA), with proximal and distal radiopaque markers pointed out with white arrows. *MVP: Microvascular plug, ASAbSA: Anterior spinal artery bearing segmental artery, ASA: anterior spinal artery, DSA: digital subtraction angiography, SA: segmental artery
Technical success was defined as the precise deployment and permanent release of the microvascular plug at the intended location following a successful test occlusion. Clinical success was defined as the absence of any clinical signs of spinal cord ischemia.
Follow-upAll patients were closely monitored and neurologically assessed as inpatients for four days following the procedure, with no temporary or permanent neurological deficits indicating spinal cord ischemia (SCI) observed throughout the entire follow-up period. Patient data were reviewed for morbidity, mortality, and complications during follow-up, extending up to six months after TEVAR. Complications were evaluated using the CIRSE Classification System.
Statistical AnalysisStatistical analysis was performed using SPSS Statistics 23.0 (IBM, New York). Continuous variables were presented as mean and standard deviation, whereas categorical parameters were presented as number and percentage. Univariable analysis of the relationship between procedural characteristics and technical (or clinical) success was assessed using Chi square and t-Tests. A two-sided-p-value < 0.05 was considered statistically significant.
留言 (0)