
記住我
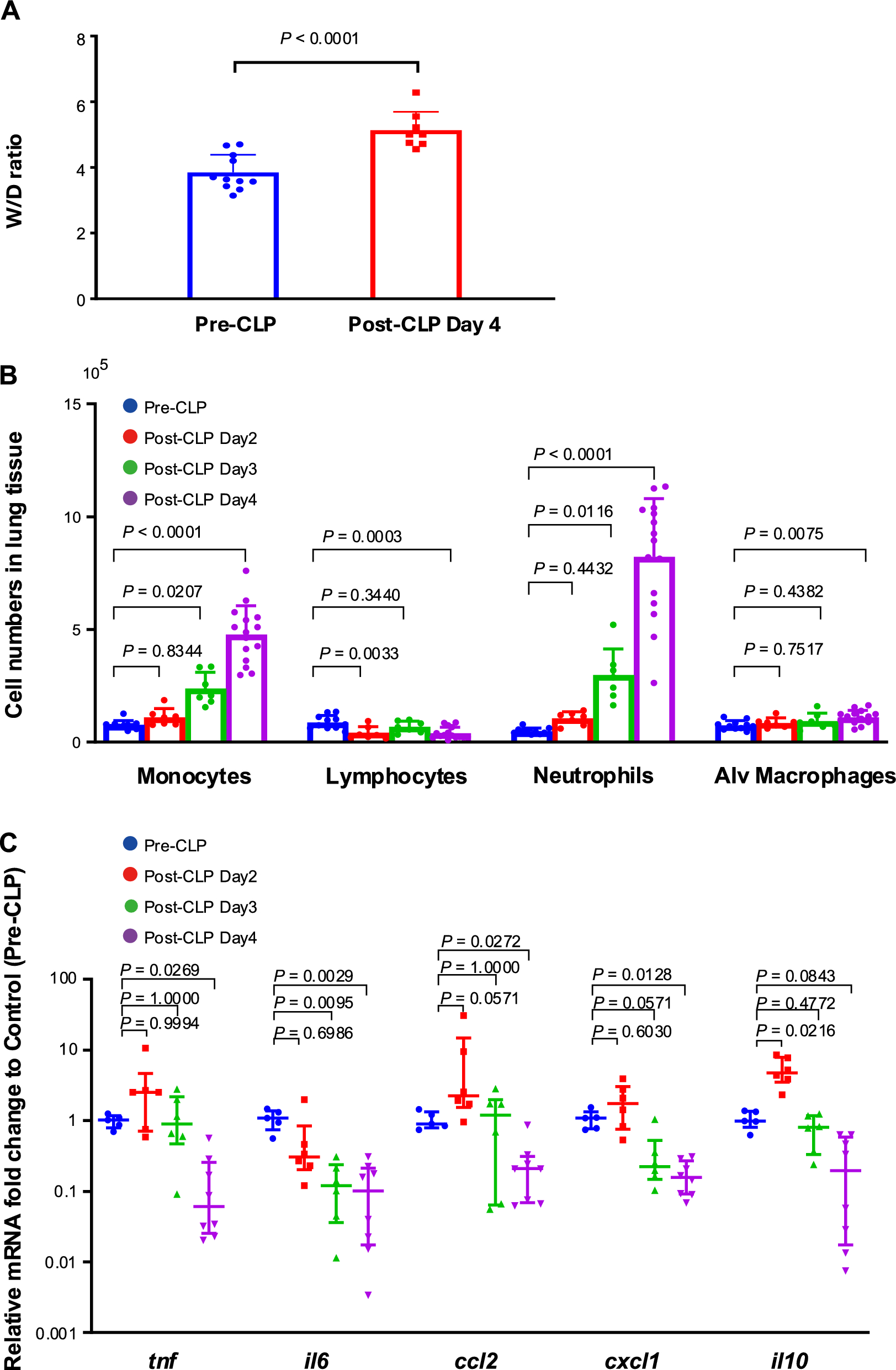
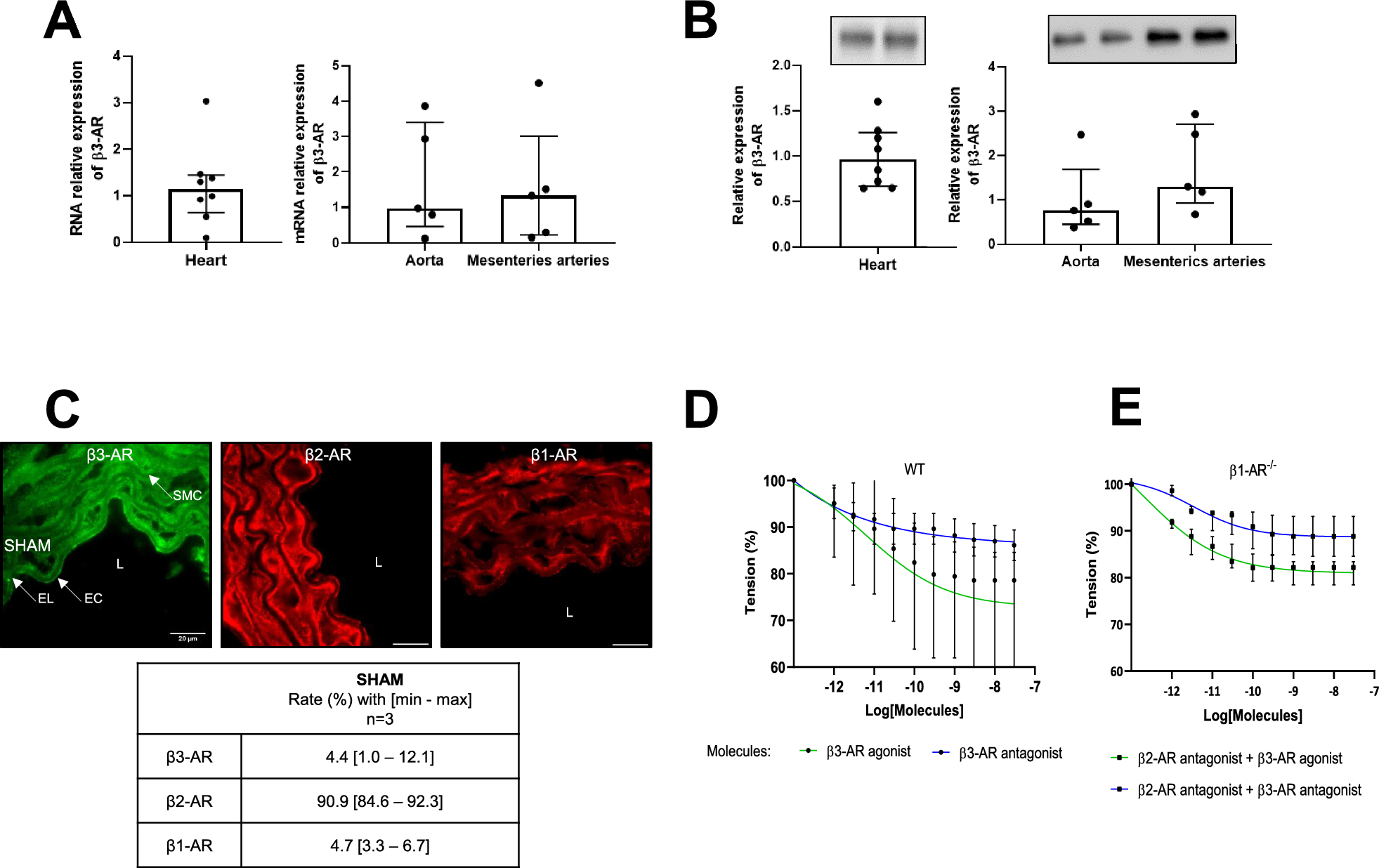
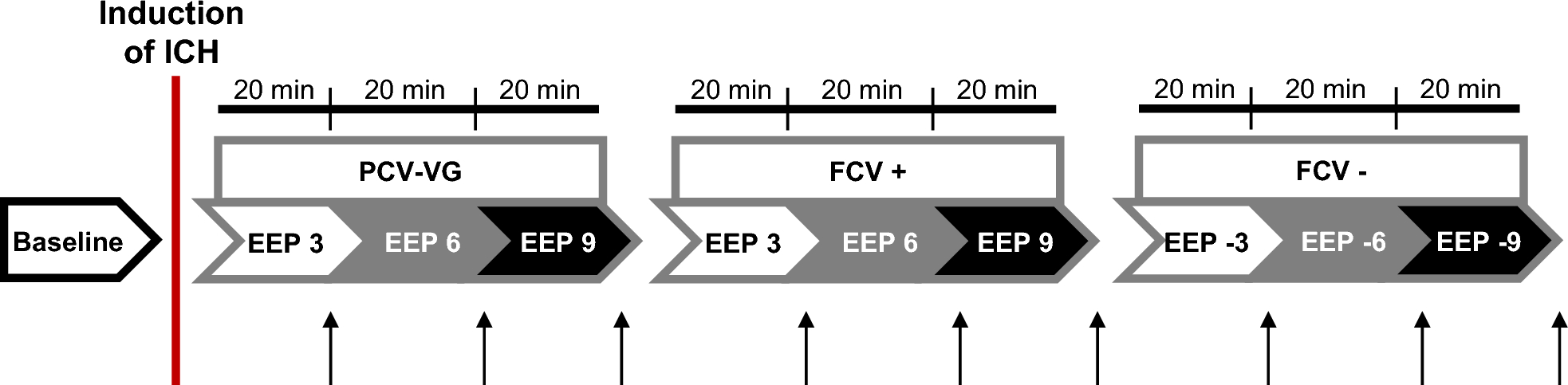
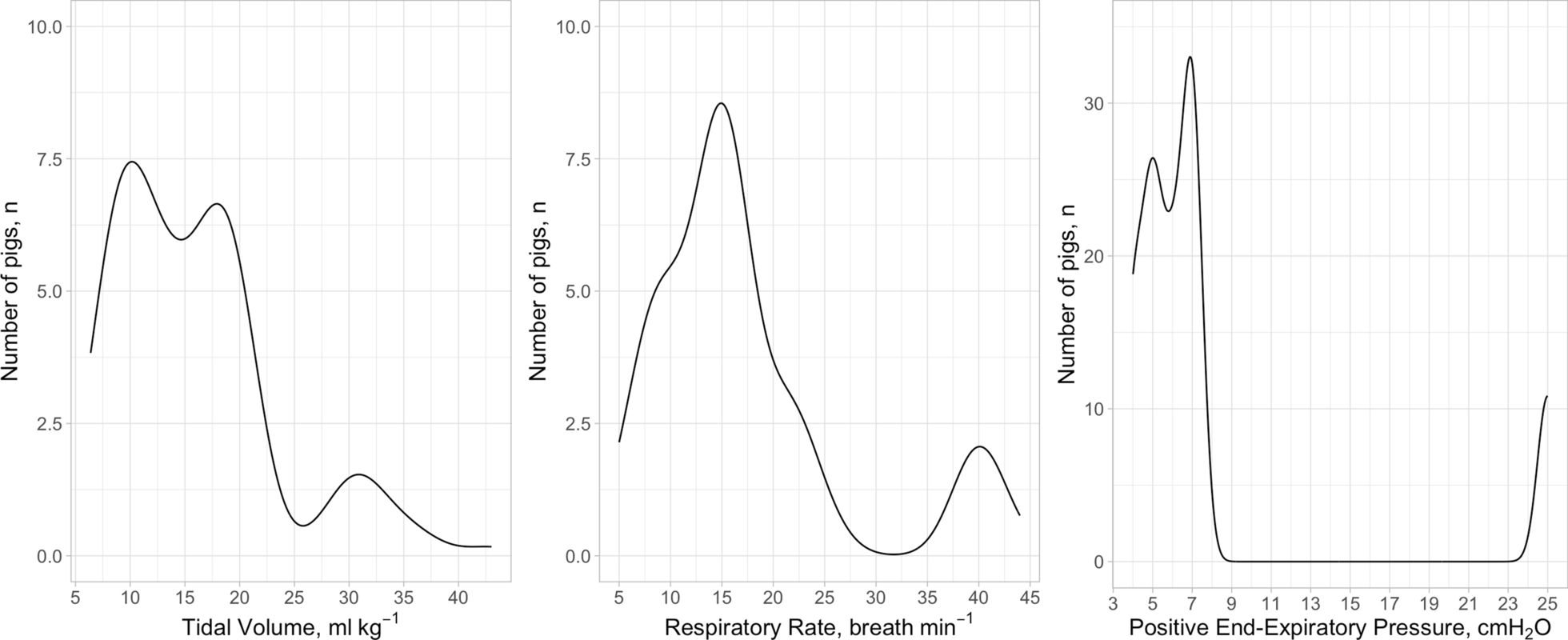





An in vitro study was conducted to investigate the effects of renal replacement therapy with and without target-controlled dialysis, using the following antibiotics: ceftazidime (CAZ), meropenem (MEM), piperacillin (PIP)/tazobactam (TAZ) (during RRT only PIP levels were quantified), vancomycin (VAN), and flucloxacillin (FXN). Furthermore, the stability of the antibiotics was tested in two common dialysis solutions. No human subjects were involved in this study, therefore ethical approval and trial registration were not required.
Experimental setupThe experiments were carried out on a MultiFiltratePRO® hemodialysis unit (the device and all disposables are manufactured by Fresenius Medical Care GmbH, Bad Homburg, Germany) in CVVHD mode. It was set up with a HDF 1000 Kit, a Polysulfone® Ultraflux® AV 1000S hemofilter (surface 1.8 \(}^2\), allows passage of molecules with a molecular weight of up to approximately 30 kDa), and multiBic® dialysis solution (Na+ 140 mmol/L, K+ 2 mmol/L, Ca2+ 1.5 mmol/L, Mg2+ 0.5 mmol/L, Cl− 111 mmol/L, \(\text _3^-\) 35 mmol/L, glucose 1.0 g/L, osmolality 296 mosmol/L), which come with standard Luer–Lock injection ports.
A simulated patient reservoir (SPR) was prepared using 10% phosphate buffer solution and 45 g/L bovine serum albumin (BSA). The SPR was stored in an Erlenmeyer flask and initially titrated to pH 7.4 with addition of 1 M HCl. Temperature was kept at 37 \(^\circ\)C, the solution was continuously mixed by a magnetic stirrer, and both pH and temperature were monitored throughout the experiment. The opening of the SPR flask was sealed with foil to prevent evaporation.
The SPR was connected to the MultiFiltratePRO® setup through polyvinyl chloride extension lines attached to the HDF 1000 kit’s tubing, leading to the hemofilter and then back into the SPR. Four standard 5 L bags of multiBic® dialysis solution were connected to the HDF kit tubing, leading to the MultiFiltratePRO® assembly and then to the hemofilter in counterflow direction against the simulated patient fluid (Fig. 1). The outflow line of the hemofilter (i.e., residual dialysate) was connected to standard Fresenius Medical Care dialysate collection bags.
Fig. 1
Representation of the experimental setup with a MultiFiltratePRO® hemodialysis unit in continuous veno-venous mode (CVVHD), setup with a hemofilter in counterflow of 1 L simulated patient reservoir (SPR) against dialysis solution (DS) from four parallel 5 L multiBic® dialysis solution bags. SPR flow (“blood flow”) \(Q_\text\) was set at 200 mL/min, dialysate flow \(Q_\text\) at 66.67 mL/min, and net ultrafiltration \(Q_\text\) at 0 mL/min
The circuit was primed using SPR instead of DS or saline solution to prevent subsequent dilution of the SPR when the circulation is activated. Roughly 10 mL of DS was required to fill the device’s drip chamber during the unit’s mandatory initialization procedure. For priming of the circuit, including the hemofilter, approximately 600 mL of SPR fluid were required, which left roughly 400 mL of SPR remaining in the SPR’s container. The primed setup is shown in Fig. 2.
Fig. 2
Experimental setup with a MultiFiltratePRO® hemodialysis unit in continuous veno-venous hemodialysis mode, primed and with both in- and outlet tubing attached to a simulated patient reservoir stored in an Erlenmeyer flask (see red rectangle) with continuous mixing by a magnetic stirrer and a heating unit. An obstacle was the machine’s blood detection sensor blocking the initiation of circulation, which was overcome by using a customized piece of cellulose-based fabric (see red arrow)
Experimental protocolThe dialysis experiment was carried out in three phases in order to reflect different scenarios, with simultaneous investigation of all five antibiotics.
Phase 1: Fresh SPR without antibiotics is dialyzed against spiked DS (i.e., containing antibiotic in TCD target concentrations). This simulates a subject with subtherapeutic antibiotic levels while being initiated on TCD. Subtherapeutic concentrations in the SPR will be increased (“up-dialyzed”) towards the target concentration.
Phase 2: The SPR is injected with a high dose of antibiotics and dialyzed against spiked DS (again containing antibiotic in TCD target concentrations). This simulates a subject with supratherapeutic antibiotic levels while being on TCD. Supratherapeutic concentrations will be eliminated towards but not below the target concentrations.
Phase 3: The dialysis solution bags are exchanged with fresh (unspiked) ones. Residual concentrations in the SPR will be eliminated towards zero, simulating traditional dialysis.
To inject antibiotics into the DS, the Luer–Lock ports on the MultiBic® DS bags were used (Fig. 3). The applied antibiotic target concentrations can be found in Table 1. During each phase of the experiment dialysis was carried out in CVVHD mode without interruption for 150 min with a reservoir flow rate (\(Q_\text\)) of 200 mL/min and a dialysis solution flow rate (\(Q_\text\)) of 66.7 mL/min, with net ultrafiltration set to zero. In between the three phases, dialysis circulation was briefly paused to change the dialysis solution as well as the residual dialysate bags, and to administer antibiotics, if required according to the protocol. From the SPR and the dialysate outflow, 2 mL samples were taken each at 0, 2.5, 5, 10, 15, 20, 30, 45, 60, 90, 120, and 150 min, during each of the three phases. In addition, initial samples were taken from the DS bags to confirm the TCD target levels. The residual dialysate bags were weighed before the procedure (empty) and at the end of each phase (full), to determine the total amount of spent dialysate.
Fig. 3
Image of MultiBic® dialysis solution bags, highlighting the standard Luer–Lock access ports, which can be used for safe and simple addition of substances for target-controlled dialysis
Table 1 Target antibiotic concentrations (mg/L) in 1 L simulated patient reservoir (SPR); concentrations (mg/L) and total amount (mg, in brackets) of spiked drug in four 5 L dialysis solution (DS) bags; for each of three experimental phasesDrug stabilityThe stability of CAZ, MEM, PIP, TAZ, VAN, and FXN in multiBic® and Ci–Ca® Dialysate K2 (Fresenius Medical Care GmbH, Bad Homburg, Germany) was investigated. The Ci–Ca® solution was not used in the dialysis experiment, but is frequently used in the critical care of patients when regional anticoagulation by citrate is applied. As a control, all substances were also dissolved in 0.9% sodium chloride solution (NaCl), which is recommended as a solvent for all tested drugs. All drugs (concentrations: CAZ and MEM: 40 mg/L, PIP/TAZ: 80/10 mg/L, VAN and FXN: 10 mg/L) were dissolved separately in 5 mL each of both dialysis fluids and NaCl, and incubated for 24 h at room temperature and ambient light. After 0, 3, 6, 12, and 24 h, an aliquot was drawn to check the solutions for any visually detectable precipitates or discolorations and to assess the pH level. Additionally, aliquots for quantification by high-performance liquid chromatography with ultraviolet detection (HPLC-UV) were drawn and immediately frozen at − 80 \(^\circ\)C to prevent further degradation of the analytes. After thawing and mixing, 10 \(\upmu\)L were injected into the HPLC system.
HPLC systemQuantification of drug concentrations was performed by two different laboratories (DF, AK: drug stability testing, CD, CL: dialysis experiments), with slightly different HPLC-UV methods.
To assess drug stability, a Shimadzu Nexera-i LC-2040C 3D system with LabSolution software (Shimadzu Europe, Duisburg, Germany) was used. Detection wavelength was 260 nm (CAZ, MEM, VAN) or 225 nm (PIP, TAZ, FXN). Separation was performed using a Nucleoshell RP18 2.7 \(\upmu\)m column (i.d. 100 × 3 mm; Macherey-Nagel, Düren, Germany). The mobile phase consisted of 0.1 M sodium phosphate buffer pH 6/acetonitrile 97.5:2.5 (v/v; TAZ), 80:20 (PIP) or 70:30 (FXN), and 0.1 M sodium phosphate buffer pH 2.6/acetonitrile 93:7 (v/v; CAZ, MEM, VAN), respectively. The retention time (flow rate 0.6 mL/min, column temperature 40 \(^\circ\)C) was 2.6 min (CAZ), 3.4 min (MEM), 4.4 min (VAN), 2.3 min (PIP), 5.0 min (TAZ) and 1.8 min (FXN), respectively.
For the analysis of the drugs in the SPR or DS from the dialysis experiments, a Shimadzu Prominence LC-20 modular system equipped with a photodiode array detector SPD M30A (Shimadzu Europe, Duisburg, Germany) was used. Detection wavelength was 225 nm (PIP, FXN), 240 nm (VAN), 260 nm (CAZ) and 300 nm (MEM), respectively. Separation of CAZ, MEM and VAN was performed using an Avantor ACE C18 3 \(\upmu\)m column (i.d. 100 × 3 mm, VWR, Darmstadt, Germany) and a mobile phase consisting of 0.1 M sodium phosphate buffer/acetonitrile 92.4:7.6 (v/v), pH 2.9. Separation of PIP and FXN was performed using a Cortecs T3 2.7 \(\upmu\)m column (i.d. 100 × 3 mm, Waters, Eschborn, Germany) and a mobile phase consisting of 20 mM sodium phosphate buffer/acetonitrile 77:23, (v/v), pH 6.5. The retention time (flow rate 0.4 mL/min, column temperature 40 \(^\circ\)C) was 4.2 min (CAZ), 5.2 min (MEM), 8.1 min (VAN), 2.3 min (PIP) and 7.6 min (FXN), respectively.
Sample preparationSample preparation for the analysis of total concentrations in the SPR (BSA solution) was performed according to a published protocol [14]. The free concentrations were measured in samples at t = 60, 120, 150, 210, and 270 min total experiment duration using a recently published ultrafiltration method prior to HPLC analysis [16]. The unbound fraction was calculated as \(f_\text = \frac}}}}\). DS was injected directly into the HPLC system. Injection volume was 1 \(\upmu\)L for all samples. The lower limit of quantification was conservatively estimated to be \(\le\) 0.25 mg/L. Based on spiked quality control samples, intra- and inter-assay imprecision as well as inaccuracy (bias) were < 8%. Regarding the free drug in BSA, accuracy cannot be specified, as the extent of protein binding in a particular sample is not known. The precision was assessed by analysing spiked BSA samples: in these samples the \(f_}\) (mean ± SD) was 99.0 ± 0.7% (CAZ), 99.2 ± 1.1% (MEM), 85.0 ± 0.4% (PIP), 79.0 ± 1.1% (VAN) and 16.0 ± 1.0% (FXN), respectively. A comparison of these values with the corresponding unbound fractions in human serum is presented in the electronic supplement, Table A1.
Data analysisData were first recorded in LibreOffice Calc 7.3 and then processed, analyzed, and plotted in Python 3 with JupyterLab 4.0 and matplotlib 3.5.2.
留言 (0)