Summary of findings
This study has demonstrated that, despite a greater reference mAs being required with use of tin filter compared with the standard filtration CRS protocol (Fig. 3), Sn100kV allows large dose savings, in standard (Fig. 4) and obese (Fig. 6) phantom sizes. Dose-savings with use of Sn100kV indicated through quantitative (Fig. 7) and qualitative (Fig. 8) assessment were in general agreement, each suggesting that large dose reductions can be made with the tin filter, and indicated that dose reductions of around 85% may be appropriate for bone imaging, whilst a 30–40% dose reduction may be appropriate for soft tissue imaging (obtained by averaging dose reductions across all soft tissues). These suggested dose reductions are supported by the sufficient comparability of the bone, lung and soft tissue image quality between the reduced-dose Sn100kV images and the full-dose CRS images in Fig. 9. The equations for the CNR vs. ED linear fits specific to tissue type provided in supplementary data Appendix I, can be used to estimate the dose reductions which can be made with use of Sn100kV, in providing comparable image quality to CRS non-tin filter images.
Whilst two studies on the use of tin filter with PET-CT have previously demonstrated that ultra-low whole-body CT doses in the region of 0.1 mSv can be used for PET AC without significantly impacting PET quantification [23, 24], this is the first study to focus on the dose reduction for L/C level CT in PET-CT, and the results should also be valid for L/C CT in SPECT-CT, provided that the same tube voltages are offered. The large dose savings demonstrated in this study are similar to those observed in tin filter studies for standalone CT for bone and lung [10,11,12,13,14,15].
Explanation of results
CNR is a widely accepted metric for evaluating image quality in CT. It is well understood that, in removing a greater proportion of lower energy photons from the X-ray beam, the tin filter provides a higher average beam energy as compared with standard filtration, if the same tube voltage is used. This in turn, is known to reduce image contrast in soft tissue and bone. With use of the tin filter at an even higher tube voltage of 140 kV, the average beam energy is considerably greater than that at 120 kV with standard filtration. Hence, the image contrast is considerably lower than the CRS scans in bone and soft tissue at Sn140kV (Fig. 5). Combined with a higher beam energy also imparting a greater absorbed dose, the noise reduction offered by the tin filter at Sn140kV is not sufficient to allow dose reduction for comparable CNR in bone and soft tissues (Fig. 5).
On the other hand, Fig. 5 shows that image contrast in bone and soft tissue is only slightly reduced at Sn100kV as compared with 120 kV with standard filtration, especially when bearing in mind that the HU scale starts at around − 1000. This phenomenon, combined with the tin filter removing such a large proportion of low energy X-rays from the beam, which are not useful to the image, means that noise is greatly reduced for the same dose, or dose can be greatly reduced for the same CNR.
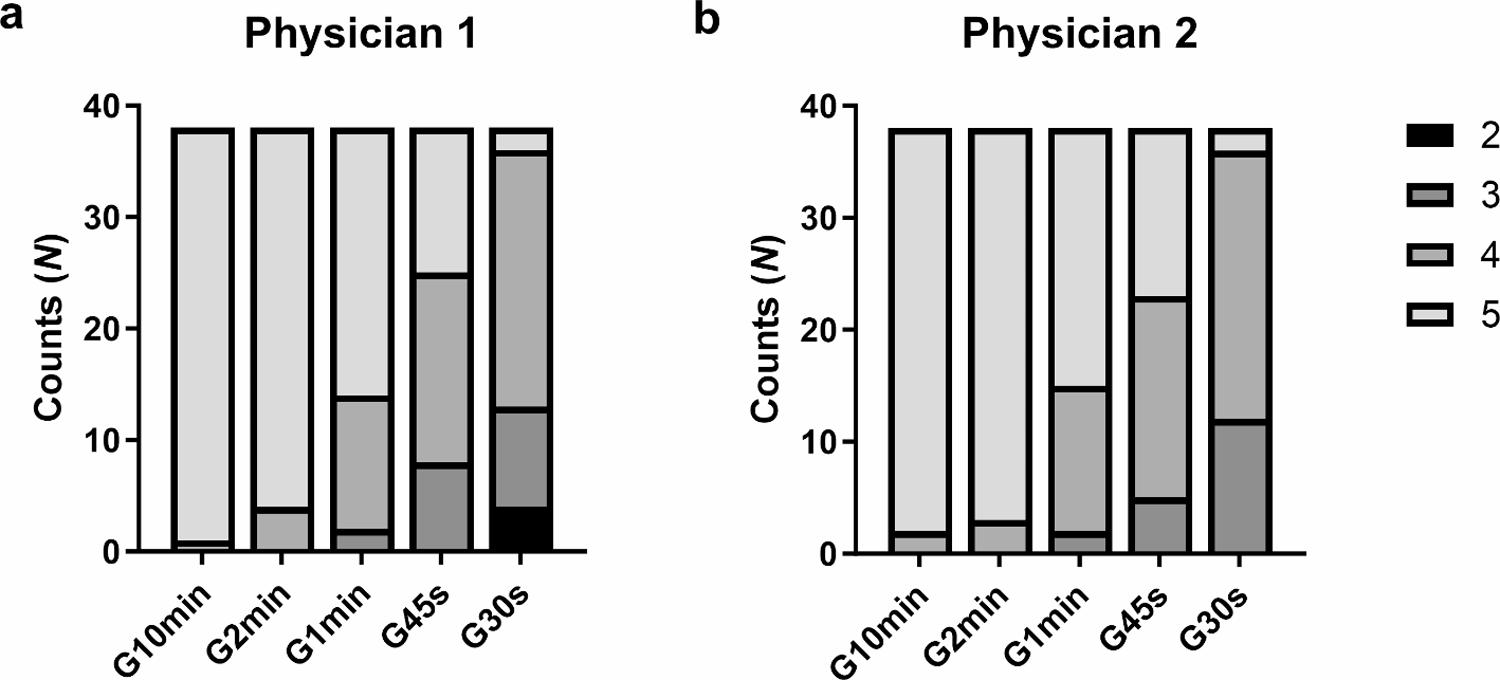
When comparing Fig. 8a and b some differences can be seen in how much dose reduction each observer deems feasible with the tin filter for comparable image quality to standard filtration scans, with observer 1 generally accepting greater dose reductions than observer 2. Still, there is clear concordance between observers that considerable dose reductions are possible using the tin filter. The permissible dose savings for bone examinations were even greater than those for soft tissue for several reasons. Firstly, greater dose savings are indicated for imaging of higher contrast structures and abnormalities, since a given level of reduction in image contrast will be less noticeable when the image contrast is already very high, as compared with a relatively low-contrast structure. Secondly, soft tissue windows tend to have a narrower HU range than bone windows, hence a small absolute difference in HU when viewed in a soft tissue window will have a greater difference in greyscale appearance and thus image contrast. Lastly, ROIs were placed in multiple soft tissues, hence there is a wider range of dose reductions seen for soft tissue, as compared with bone which was represented by just one ROI. That said, the suggested dose-savings for soft tissue examinations were still large, albeit not as large as for bone.
Clinical implementation
The data from this study suggests that CT dose reductions in the region of 30–40% and 85% can be made for soft tissue and bone examinations, respectively, for comparable L/C CT image quality to CRS protocols with standard filtration. On this basis, an 85% dose reduction has been implemented in clinical practice for L/C CT in NaF PET-CT with use of the Sn100kV/50 mAs setting in this department, given the excellent bone image quality at such marked dose reduction. For implementation of the suggested dose reductions in soft tissue imaging, such as for FDG PET-CT, the authors feel that a more careful clinical validation is necessary to compare visualisation of lymph nodes and metastases between dose-reduced tin filter and standard filtration scans.
Previous studies have shown that down to 0.1–0.2 mSv whole-body CT dose in a standard-sized patient or phantom (Sn100kV with 25–50 mAs) the impact on PET AC is negligible [23, 24]. If implementing an 85% dose reduction for bone examinations, the soft tissue CT visualisation in the bone scan may be inferior to the CRS protocol, since such an aggressive dose reduction is not indicated for soft tissue. However, for optimisation of CT image quality and radiation dose, the clinical purpose of the CT scan should be borne in mind. For example, in the case of bone imaging with 18F-NaF PET-CT at this Nuclear Medicine department in which an 85% CT dose reduction has been made with the tin filter, visualisation of bone and not lymph nodes, is the clinical purpose of the CT scan.
The findings in this study describe only the CT dose-savings possible with use of the tin filter. However, the PET-CT systems offering tin filter technology are also equipped with a state-of-the-art Stellar detector, which reduces noise thereby allowing dose reductions of 27-70% depending on tissue type [25], as well as large dose reductions offered by the second and third generation iterative reconstructions [26,27,28]. Even prior to implementation of the tin filter, this department’s 120 kV/20 mAs CRS L/C CT scan for 18F-NaF bone PET-CT examinations (1.4 mSv in a standard-sized patient), was already less than half of the reported Nordic median dose [4]. With the addition of the tin filter reducing this dose to just 0.2 mSv in a standard-sized patient, this department is delivering a CT dose for 18F-NaF PET-CT at a greater than 90% reduction compared with the Nordic median dose.
These combined state-of the-art CT technologies allow such low CT radiation doses in PET-CT, that in addition to reducing the supposed risk of inducing a fatal cancer in later life for patients already undergoing PET-CT, these greatly reduced CT doses can also potentially change molecular imaging practice. For example, we may see a greater transition from planar gamma camera to cross-sectional hybrid imaging, since lesion detection (sensitivity) is greater [29, 30] and the lower radiation dose is more easily justifiable. Furthermore, PET-CT may be more justifiable for younger populations and pregnant patients [31], instead of referrers being persuaded to choose lower-dose alternatives.
Study design
This study examined CT dose reductions possible with the tin filter for L/C level CT image quality in PET-CT, compared with the CRS. For simplicity, all protocols used CARE kV in ‘semi’ mode, meaning that a fixed CT tube voltage was used, rather than utilising the full CARE kV functionality to optimise tube voltage specific to patient/phantom size, as is performed clinically in this department. Previous phantom acquisitions (data not shown) suggest that 100 kV is deemed optimal by the CARE kV application for the standard phantom configuration, and 120 kV for the obese configuration. Whilst tube voltage optimisation with CARE kV for the CRS scan would have resulted in no dose differences for the obese phantom, it may have reduced dose in the standard-sized phantom, with a previous study demonstrating up to 9.3% dose reduction with an optimal tube voltage of 100 kV in phantoms [32]. However, even assuming the full 9.3% dose reduction could be realised in the CRS scan through tube voltage optimisation at 100 kV, this would have contributed little difference to the observed relative dose savings with the tin filter (around 1% difference for bone and 7% for soft tissue).
The methods section details that scan settings were optimised for bone image quality, with the CARE kV sliding bar setting set to the bone exam type, and choice of the spine organ characteristic for tube current modulation, since this department was most interested in implementing the tin filter for 18F-NaF bone PET-CT from the outset. However, these settings would have no impact on the relative dose savings between tin filter and CRS scans with standard filtration, or the absolute dose required to achieve a given level of image quality, in any tissue type.
This study reported relative dose savings which could be made with the tin filter as compared with standard filtration protocols for comparable image quality, and the absolute effective doses which would have been delivered to a patient, by use of a whole-body multiplication factor to convert DLP to ED in standard-sized patients, as described by Inoue et al. [21]. AAPM Report 204 describes the influence of patient size on absorbed dose, with smaller patients incurring a greater absorbed dose and larger patients incurring a lower absorbed dose, for a given scanner output. This can lead to absorbed doses and thus effective doses being underestimated in smaller patients and overestimated in larger patients. To remedy this, SSDE conversion factors were published in AAPM Report 204, to allow normalisation of absorbed dose values for patient size. Yet, the dose values presented in this study had not been normalised for size, since the published conversion factors are applicable only to the thorax-abdomen-pelvis scan range and not for the vertex-to-knee scan range used in this study. This phenomenon has no impact on the relative dose reductions achieved with tin filter protocols as compared with standard filtration protocols for comparable image quality. However, it should be borne in mind that the absolute effective doses quoted for the obese configuration may be overestimated in this study, and the absolute doses for the standard phantom may be slightly underestimated.
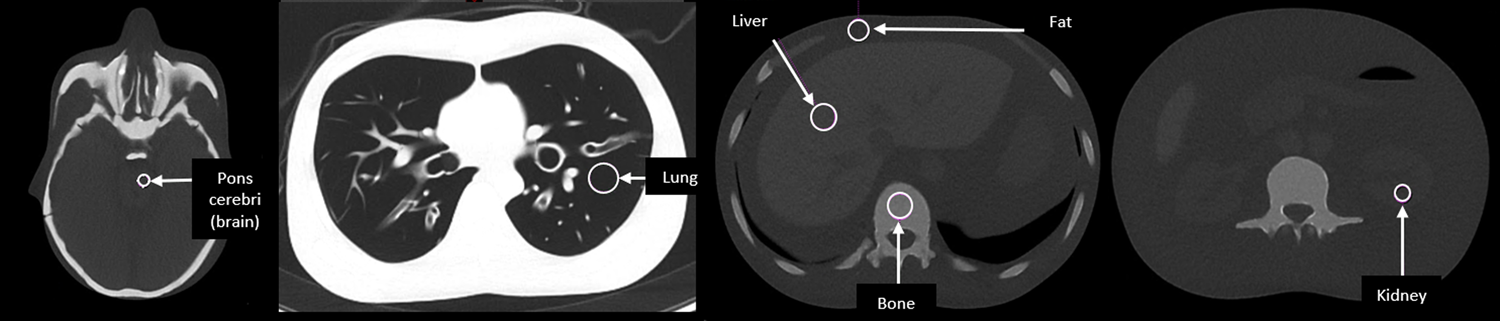
A ROI placed in fat was used in this study as a reference for measuring contrast. In this phantom, this is placed in an area which in a real patient may comprise a mixture of fat and muscle. Hence, if calculating CNR in a patient, a different reference region may be required.
This investigation has not addressed the potential impact on PET images, when using a CT scan for PET AC acquired using the tin filter at the investigated settings. However, previous work has demonstrated that with Sn100kV at the mAs settings advocated for in this study (minimum 50 mAs), there is a < 2% difference in PET quantification at soft tissue and bone equivalent densities [23].
Limitations and future work
This study evaluated image quality in a phantom with normal morphology, without representation of abnormalities typically seen in clinical PET-CT examinations. Imaging of the PBU-60 phantom is an adequate and ethical means to assess differences in dose and image quality in the human body when comparing different CT exposure settings. Nevertheless, a patient-based study validating the clinical adequacy of real patient images exhibiting adequate visualisation of real clinical abnormalities would provide additional reassurance for implementing these dose reductions with use of the tin filter in clinical practice.
In this study, the doses and image quality provided by the tin filter were investigated at the two available tube voltages: Sn100kV and Sn140kV. However, other CT systems may have other tin filter tube voltages available. This study has demonstrated that the dose and image quality delivered by the tin filter is highly dependent on the tube voltage, and thus, further studies should be undertaken to evaluate the dose reductions which can be made with the tin filter at the other available tube voltages.
This study only compared dose savings with tin filter for comparable CNR and visual interpretation but did not evaluate differences in artefacts between tin filter and standard filtration scans, which should be evaluated in future work. Lastly, this study only compared dose savings with the tin filter in adult body sizes, and future work should also evaluate the possible dose savings with the tin filter in paediatrics.







留言 (0)