
記住我




Here, we describe a case of colonoscopic incarceration of an inguinal hernia managed manually under fluoroscopic guidance. Our findings demonstrate that emergency surgery can be avoided, and beneficial treatment can be provided in such cases.
Although colonoscopy is commonly performed, the colonoscopic incarceration of an inguinal hernia is rare. Since the first report by Leisser in 1990, only 24 cases have been reported, including ours (Table 1) [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]. All reported cases involved older male patients, and 23 of the 24 patients had hernias on the left side. We speculated that the reason all cases involved men was the significantly higher risk of hernia development in them due to anatomical differences. In men, the inguinal canal is slightly wider due to the passage of the spermatic cord, resulting in a hernia risk approximately 9 times higher than in women. Furthermore, the risk increases with age as supportive tissues weaken, leading to enlargement of the hernia opening [22]. The reason for this left-sided predominance is speculated to be the pressure exerted by the insertion and withdrawal of the colonoscope. One patient with right-sided incarceration was diagnosed after a right hemicolectomy for diverticular bleeding, suggesting that surgery-induced anatomical changes or adhesions may affect bowel positioning [4]. In addition, more than half of the patients had undiagnosed hernias before the colonoscopy. Inguinal hernias are common among older men, with a prevalence of 6% [23]; however, without patient-reported symptoms, detection before colonoscopy can be challenging. In our patient, if an inguinal hernia had been detected before the colonoscopy, incarceration of the colonoscope in the hernia and subsequent procedural interruption could have been prevented. Although the patient’s surgical history is crucial, verifying the presence of a hernia before colonoscopy is vital. Furthermore, previous reports have indicated relative contraindications for colonoscopy in the presence of large inguinal hernias, necessitating a discussion of the associated risks [4]. Computed tomographic colonography is the recommended alternative when colonoscopy is necessary prior to hernia repair. When colonoscopy is essential, such as when a malignancy is suspected, the risk of incarceration is reduced by manually reducing the hernia and maintaining bowel straightening during colonoscopy [14]. In our case, colonoscopy was performed after hernia repair because the tumor was not suspected.
Table 1 Summary of reports on colonoscopic incarceration of inguinal herniasReduction under fluoroscopic guidance has become increasingly common, and cases of emergency surgery have been reported due to extraction difficulties [7, 12, 16, 17, 19]. An effective reduction technique must be devised to manage colonoscopic incarceration based on a thorough understanding of its mechanism. To date, incarceration has occurred either during insertion (n = 17, including the present case) or withdrawal (n = 7) of the colonoscope. The size of the hernial orifice and the extent of adhesion can influence incarceration, which can lead to entrapment of the bowel and mesentery. During withdrawal, the colonoscope may form a loop originating from the hernia orifice, suggesting potential entrapment. If loop formation does not occur, manual straightening of the colonoscope can facilitate the reduction. However, when loop formation occurs, forced reduction may lead to perforation because the colonoscope and bowel may become trapped in the arcuate portion. In such cases, the pulley technique, which involves grasping the loop arc while withdrawing the colonoscope, has proven to be effective (Fig. 2a, b) [4]. In our patient, the absence of loop formation confirmed under fluoroscopic guidance allowed for successful reduction using manual pressure, and follow-up contrast enema showed no signs of perforation. We believe that by effectively utilizing imaging studies without forced reduction, emergency surgery can be avoided and definitive endoscopic surgery performed.
Fig. 2
Mechanism of colonoscopy incarceration and reduction techniques. a No loop formation. Straightening the colonoscope with manual pressure can facilitate reduction. b Loop formation. The pulley technique, wherein the loop arc is grasped when the colonoscope is withdrawn, is effective
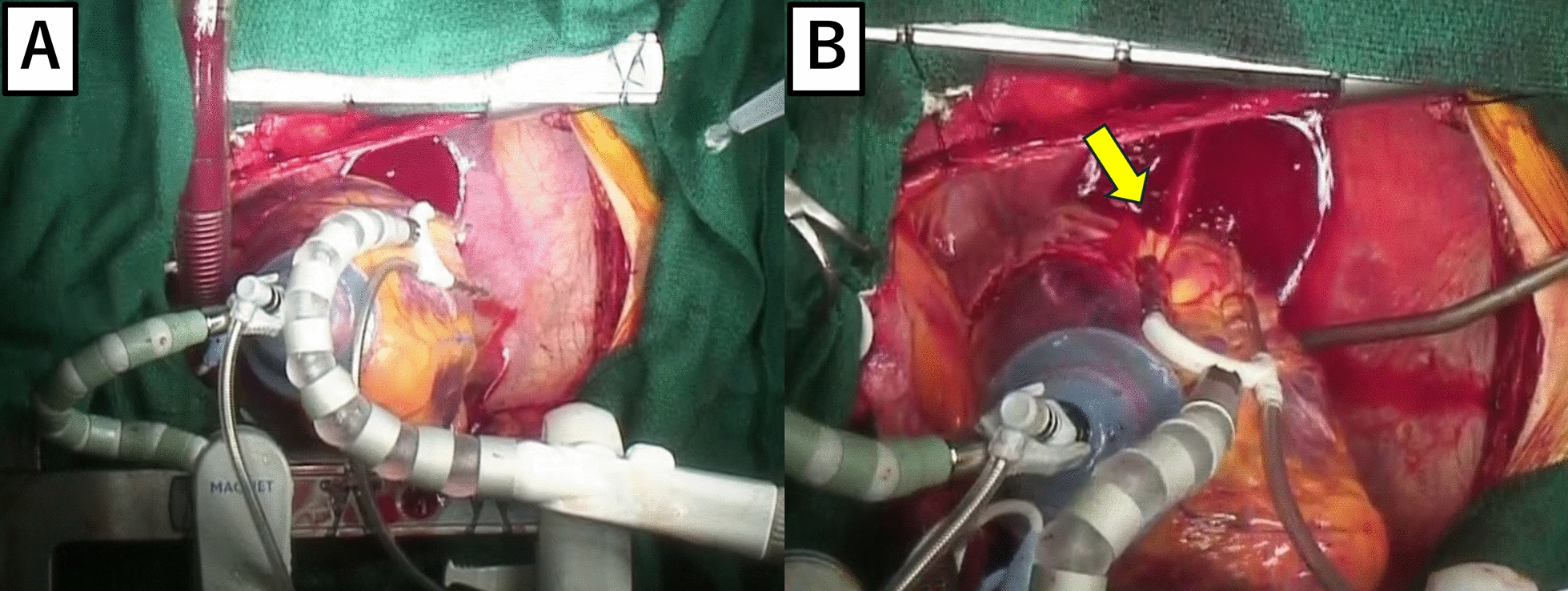
Although surgery depends on the patient's preference, definitive surgery is often performed 2–3 months after successful manual reduction, and we followed the same approach in this case. Intraoperative findings revealed a left direct inguinal hernia with the sigmoid colon incarcerated within the hernia sac. Additionally, extensive sheet-like adhesions around the hernia orifice were observed, which were likely formed due to repeated prolapse over time. Based on those findings, we determined that the intraperitoneal surgery would be difficult, and opted for the extraperitoneal approach. Our strategy suggest that a total extraperitoneal hernia repair can be safely performed without damaging the intestinal tract.
留言 (0)