The most common cause of ectopic pancreas is generally believed to be stray pancreatic tissue during fetal development. In addition, the most common sites of ectopic pancreas are the duodenum and stomach, which are close to the pancreas, followed by the jejunum, ileum, and Meckel’s diverticulum [5]. The condition predominantly affects males, with a male-to-female ratio of 2:1. Typically, ectopic pancreas does not present with clinical symptoms. Moreover, Heinrich classification [2] is a well-known tissue classification method. Type I has islets of Langerhans, adenocytes, and conduits and has the same structure as normal pancreatic tissue; type II lacks islets of Langerhans and comprises adenocytes and conduits; type III lacks islets of Langerhans and adenocytes and comprises only conduits; and type IV comprises only islets of Langerhans without pancreatic exocrine tissue. Based on pathological findings, our case was classified as Heinrich type II.
Although multiple reports of ectopic pancreatic carcinogenesis exist in the past, our review of the Non-Profit Organization (NPO) Japan Medical Abstracts Society database from 2000 to 2023 under the terms “jejunum” and “ectopic pancreatic cancer” revealed 22 reports, including our cases. However, the only reported cases discovered as a result of bowel accumulation were our self-examined cases (excluding conference proceedings).
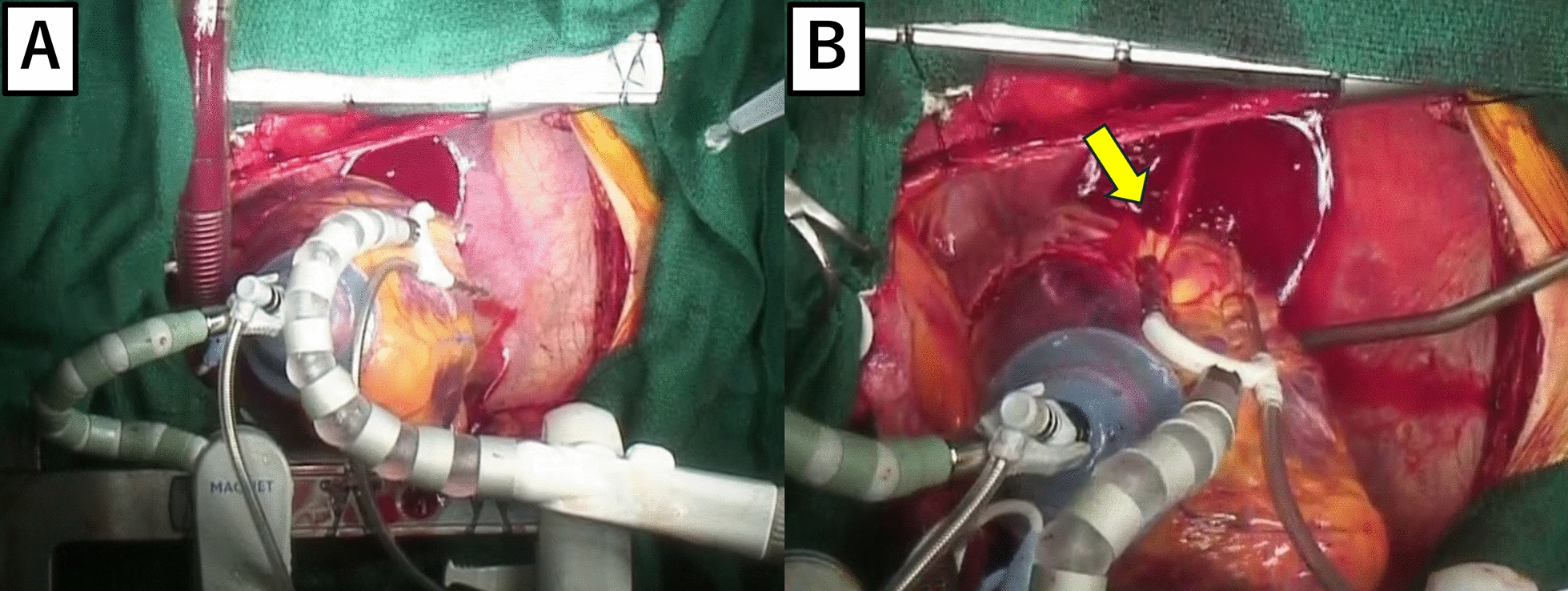
The criteria for the transformation of the ectopic pancreas into carcinoma, according to Mibayashi et al. [6], are as follows: (1) the lesion must be observed grossly, mainly from the submucosa to the muscularis mucosae, and show no association with the mucosa except for mucosal perforation; (2) the ectopic pancreas must be complicated or coexist, and the tumor must show evidence of a transition from these lesions to carcinoma or the histological picture of the tumor must resemble that of pancreatic cancer; and (3) the tumor must not have metastasized from pancreatic cancer. In this case, the patient was found to have intestinal accumulation, and the intraoperative specimen was opened due to suspicion of jejunal carcinoma exposed on the mucosa. Therefore, the lymph nodes of the patient were dissected.
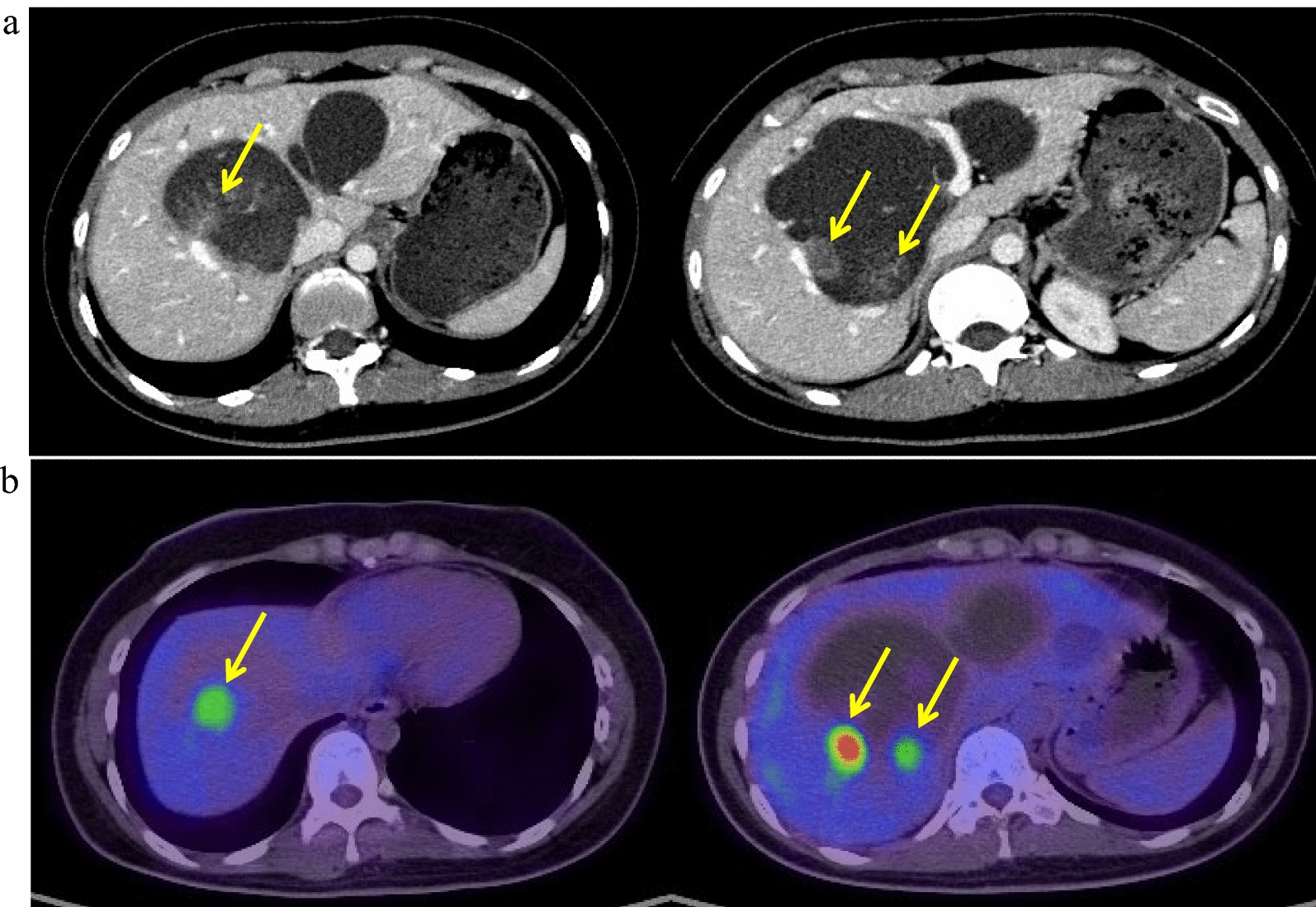
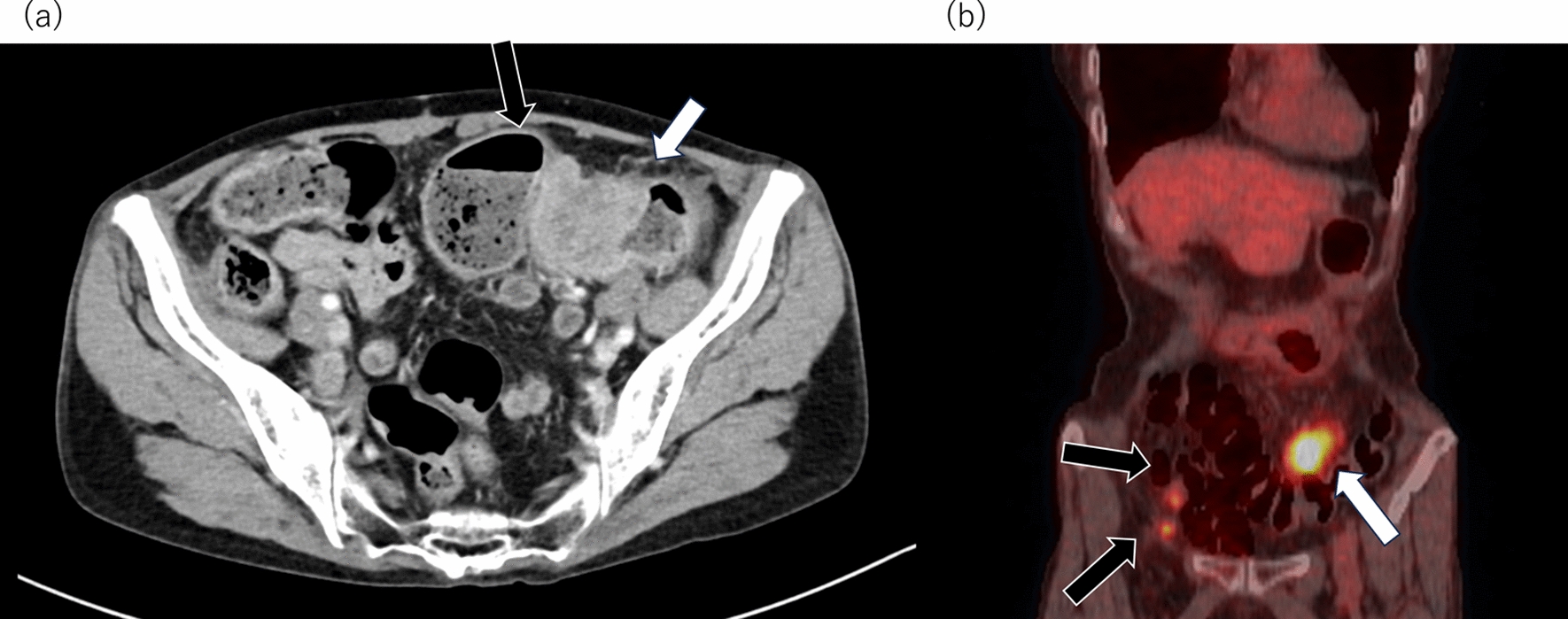
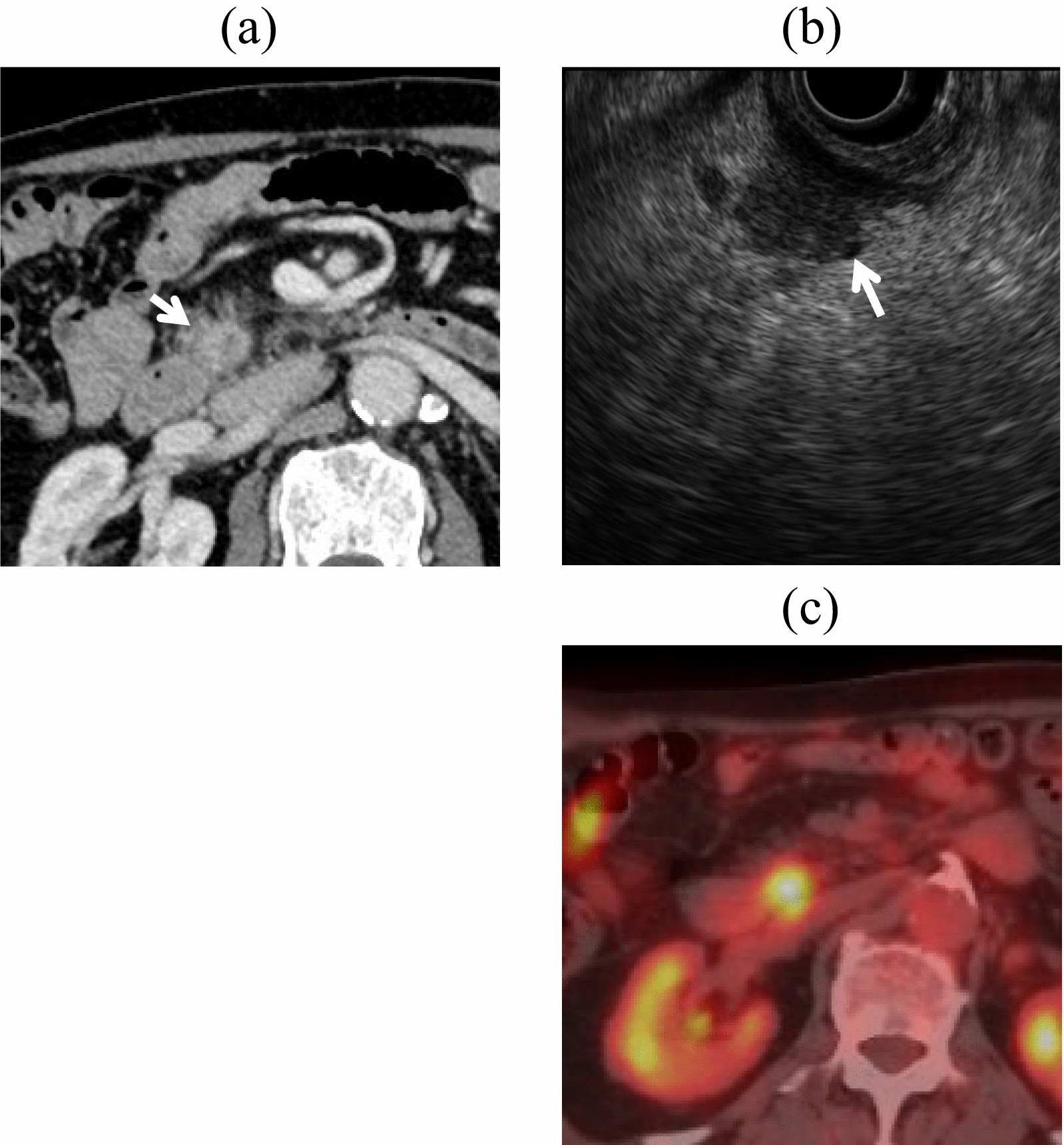
In this case, the pathological findings showed a Heinrich type II ectopic pancreas and a tumorigenic image of the pancreatic duct, mainly in the submucosal layer, extending from the abrupt transition part of the mucosal surface to the intrinsic muscular layer. As the contrast-enhanced CT scan showed a normal pancreas, we considered that the case met the definition of ectopic pancreatic cancer of the jejunum. The size was 3.5 cm, depth was in the intrinsic muscular layer, and no lymph node metastases were observed. According to previous literature, 80% of lesions are 1–3 cm in size, and most of them are located from the submucosa to the muscularis propria [7]. When diagnosed with ectopic pancreatic cancer, Hirata et al. [8] recommended treatment according to pancreatic cancer based on histological features. The need for lymph node dissection, in addition to lesion resection, has been highlighted.
According to the National Cancer Center and Rare Cancer Center website [4], small intestine cancer generally refers to duodenal, jejunal, and ileal cancers, with neuroendocrine tumors, adenocarcinomas, malignant lymphomas, and sarcomas (gastrointestinal stromal tumors and leiomyosarcoma) as the most common histologic types. It is considered a rare type of cancer, accounting for < 0.5% of all malignant tumors and < 5% of all malignant gastrointestinal tumors. Small intestinal adenocarcinoma is staged according to the UICC-TNM classification, although its treatment has not yet been established. While resection of the lesion is a curative treatment, the need for dissection and the resecting area is yet to be clearly elucidated. Moreover, the effectiveness of adjuvant chemotherapy after radical surgery has not been established, and no drugs are covered by insurance. The efficacy of fluoropyrimidine + oxaliplatin therapy has been demonstrated in stage IV patients with distant metastases or recurrent disease, and fluorouracil, leucovorin, and oxaliplatin (FOLFOX) is also covered by insurance in Japan. However, only approximately 10% of a relatively high rate of MSI-positive patients are known, and the efficacy of pembrolizumab has been demonstrated.
Hoshino et al. [1] reported 20 cases of ectopic pancreatic cancer of the jejunum. A total of 22 cases exist, including our case. Among these, eight cases had lymph node metastasis or distant metastasis at surgery, and eight experienced recurrence within 1 year after radical resection, all with a poor prognosis. All patients were treated with chemotherapy according to the guidelines for pancreatic cancer treatment. In addition to the study by Miyazaki et al. [9], eight cases of so-called N0 and M0 have been reported, as in the present case, although the exact staging was difficult to determine as the depth of some cases was unknown. Moreover, the optimal duration of chemotherapy administration is unknown. Table 1 presents the postoperative recurrence and survival of these seven patients with early-stage cancer, with or without adjuvant chemotherapy. Our patient did not receive postoperative adjuvant chemotherapy but survived 24 months postoperatively without recurrence.
Table 1 Past reported cases of adenocarcinoma of ectopic pancreas in the jejunumS-1 and gemcitabine (GEM) are recommended as adjuvants for pancreatic cancer [10, 11]. As mentioned above, no clear evidence of small intestinal cancer exists. If jejunal ectopic pancreatic cancer is treated as pancreatic cancer, S-1 or GEM would be the treatment of choice. Miyazaki et al. [9] suggested the efficacy of adjuvant S-1 as well as pancreatic cancer. In our case, adjuvant therapy was indicated as the treatment of choice because the pathological findings revealed a tumor with vascular invasion. Although we recommended S-1 as a first choice, we decided to follow up without adjuvant therapy as per the patient’s choice. Fortunately, the disease has not recurred, although we are still carefully monitoring the patient’s progress, partly due to the abovementioned reasons.
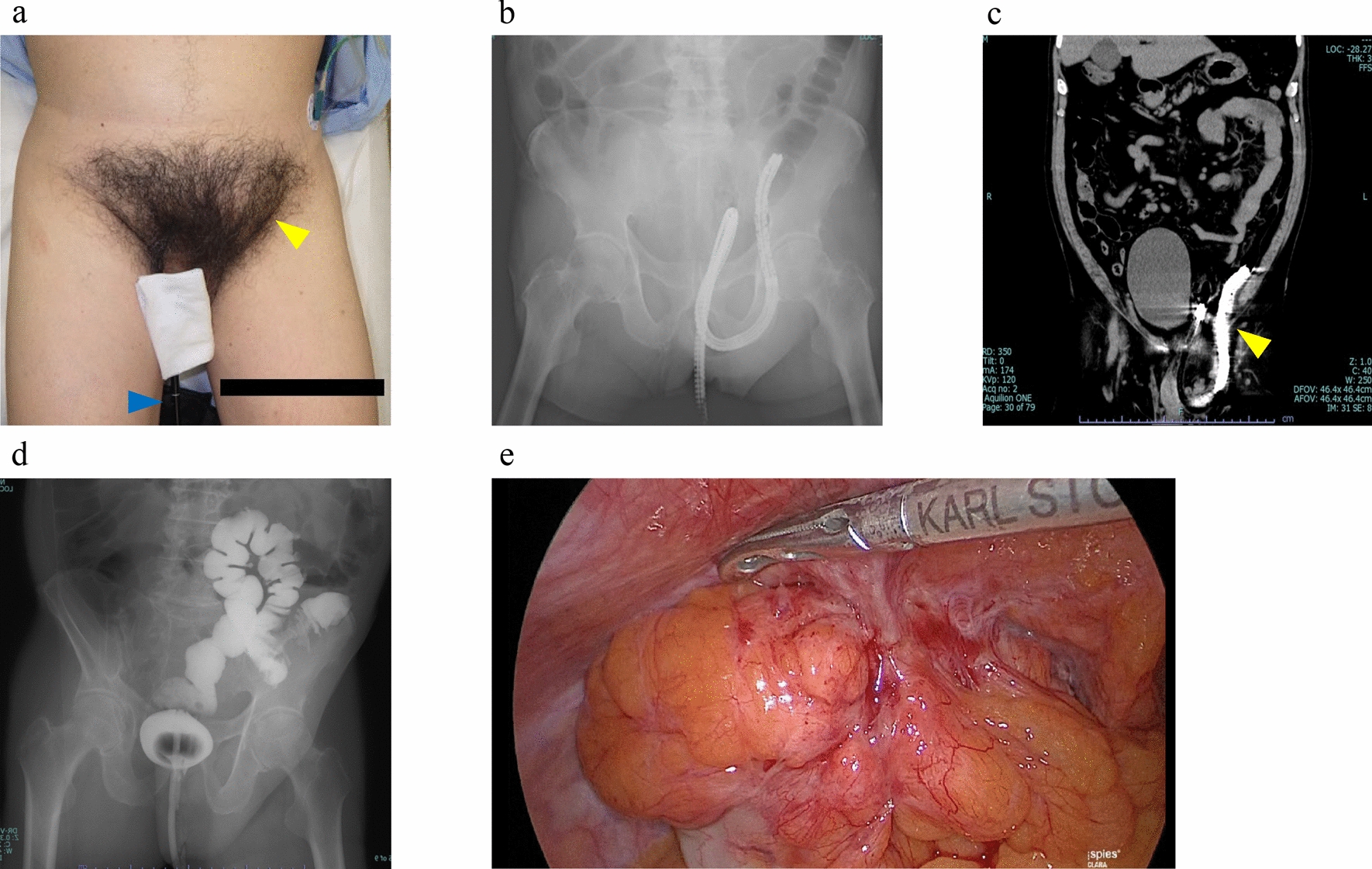
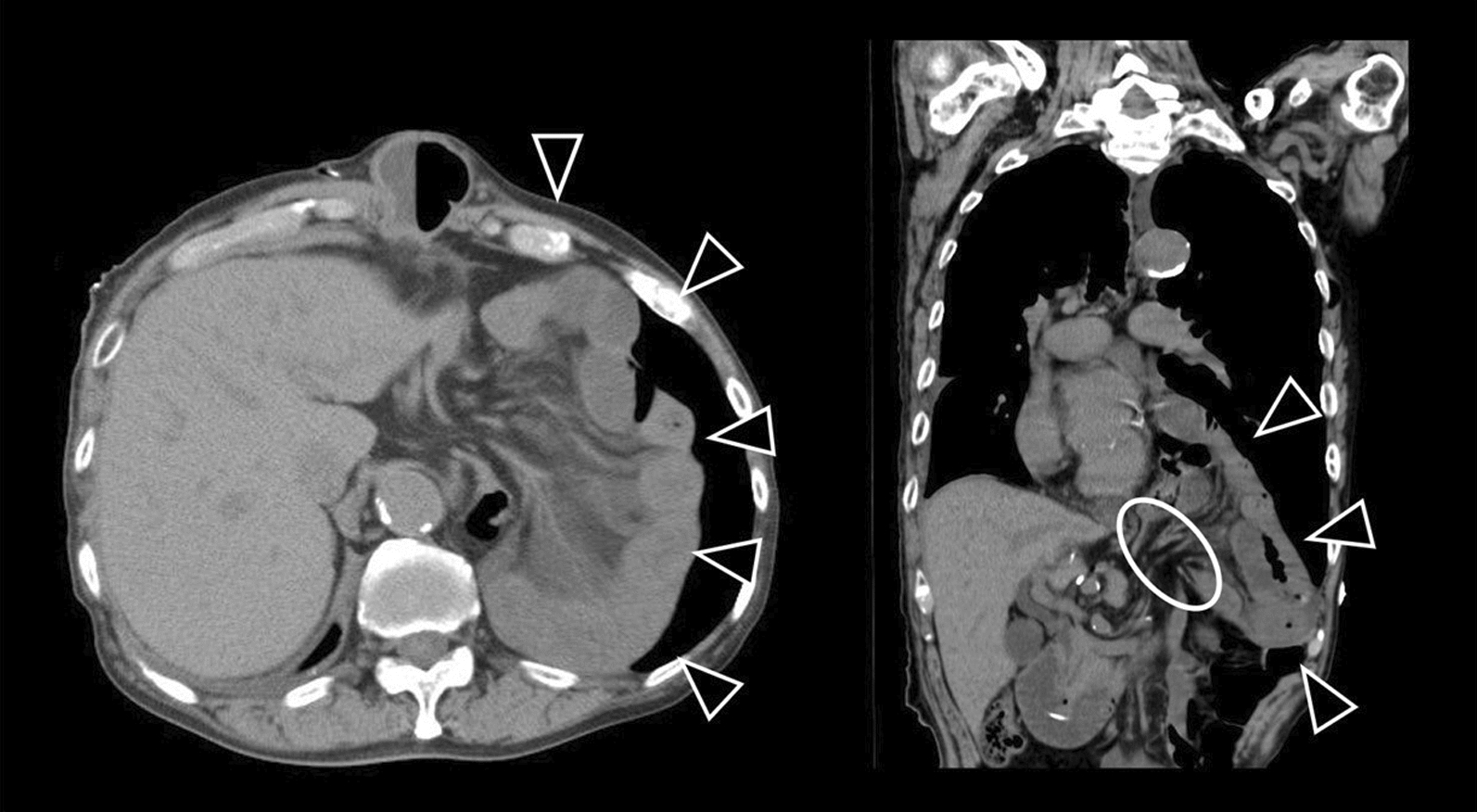
In the case of advanced pancreatic cancer, other options are available in accordance with the guidelines for pancreatic cancer treatment; however, the prognosis is extremely poor, even in the cases reported to date. Therefore, as with pancreatic cancer, early detection of ectopic pancreatic cancer is required; however, similar to tumors of the small intestine, it takes time for symptoms to appear. Previously, many patients visited hospitals with abdominal pain and nausea, and intestinal obstruction was found upon close examination. In our case, the patient had a stacked intestine, although the cause of vomiting associated with dilatation of the oral intestinal tract was the same.





留言 (0)