
記住我




An 80-year-old man with acute heart failure was admitted to another hospital. He had previously undergone percutaneous coronary intervention but had self-discontinued medications including aspirin. After oxygenation improved with diuretics, coronary angiography revealed triple-vessel disease. Transthoracic echocardiography showed severe left ventricular dilation (diastolic dimension 60.8 mm, systolic dimension 57.2 mm) with an ejection fraction of 21.6%. Mild-to-moderate mitral regurgitation and a left atrial volume index of 45.8 mL/m2 were noted. He was recommended to undergo CABG and was transferred to our hospital. We planned isolated CABG and Mitral regurgitation was mild on reexamination, mitral valvuloplasty was omitted.
After median sternotomy, bilateral internal thoracic arteries and the saphenous vein Graft (SVG) from the left lower leg were harvested. Heparin (300 IU/kg) was administered after opening the pericardial cavity. An Acrobat heart positioner (Getinge, Gothenburg, Sweden) and an OPHIDIA stabilizer (VITAL, Tokyo, Japan) were used for coronary artery exposure. In order to anastomose to the obtuse marginal branch (OM), the right internal thoracic artery (RITA) was passed through the transverse pericardial sinus. Although an attempt was made to perform OPCAB at first, the hemodynamic condition gradually deteriorated with heart disposition and transesophageal echocardiography revealed moderate to severe mitral regurgitation. We decided to perform on-pump beating CABG. A cardiopulmonary bypass was initiated and the anastomosis between RITA and OM was performed uneventfully.
Next, to expose the right coronary artery, the positioner was attached to the apex of the heart, and the heart was transposed to the caudal side (Fig. 1A). When anastomosis between the posterior lateral ventricular branch (PLV) and SVG was about to start, sudden massive bleeding occurred in the pericardial cavity. A 2-cm-long laceration was found on the posterior wall of the left atrium between the atrioventricular groove and the left inferior pulmonary vein (Fig. 1B). A left ventricular vent was inserted and the amount of hemorrhaging was decreased. The first repair was attempted from the epicardial side using felt strips but was unsuccessful. The Heart was gone under cardioplegic arrest, the left atrium was then opened through a transseptal approach. A 5-cm fissure was found beside the posterior mitral annulus (Fig. 2A) and repaired with an oval bovine pericardial patch using 4-0 polypropylene continuous sutures (Fig. 2B). Despite intact mitral valve leaflets, substantial regurgitation was observed on the water test, necessitating annuloplasty with the tailor flexible annuloplasty ring (Abbott, Illinois, U.S.). The left and right atrium were closed, and then the remaining CABG was completed under cardiac arrest. Finally left internal thoracic artery to left anterior descending artery, RITA to OM, SVG to Diagonal branch, and SVG to the posterior descending artery and PLV were performed. SVGs were anastomosed to the ascending aorta. Since the RITA was interfering with the hemostasis of the left atrium, it was divided at the root and formed into a V-composite with the SVG anastomosed to a diagonal branch. Cardiopulmonary bypass was weaned off with intra-aortic balloon pumping assistance. The operation, extracorporeal circulation, and aortic clamping times were 474, 240, and 142 min, respectively.
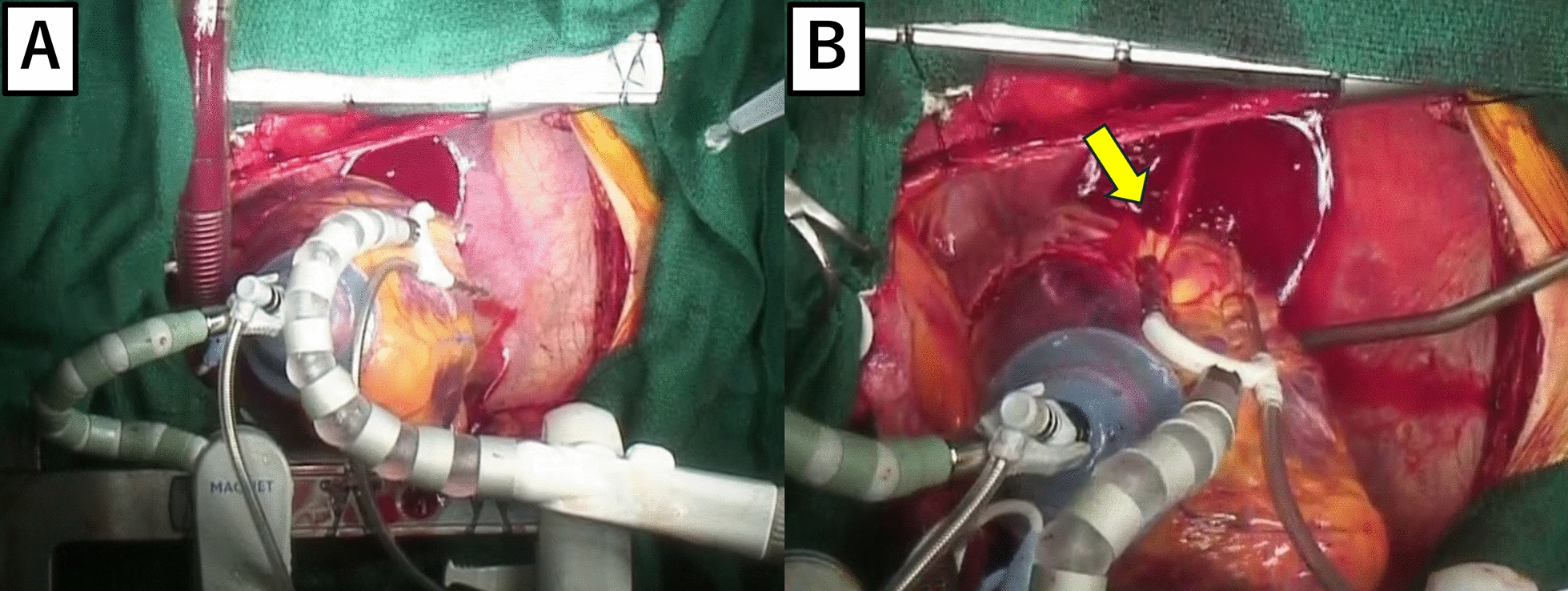
Fig. 1
Intraoperative findings from outside the heart. A Just before atrial rupture, the heart was displaced cranially using a vacuum device. B There was a 2-cm laceration on the posterior wall of the left atrium and bleeding (arrow)
Fig. 2
Intraoperative findings in the left atrium before and after repair. A Inner side of the left atrium. A 5-cm tear along the mitral annulus (arrowhead). B The rupture site was repaired using a bovine pericardial patch. The suture line (arrowhead) was close to the mitral annulus (arrow)
Postoperatively, continuous hemodialysis was temporarily administered. However, he was transferred to the ward after 10 days. Computed tomography showed patency of all grafts and no pseudoaneurysm in the left atrium. An echocardiogram performed after 3 months showed that the left ventricular ejection fraction was 34% and mitral regurgitation was trivial.
留言 (0)