PAPVC is a rare congenital vascular anomaly; its frequency is estimated at 0.4–0.7% in postmortem examinations [2]. Notably, PAPVCs are usually detected in the right lung, with only 10% of anomalies occurring in the left lung [2]. Furthermore, 80% of PAPVC cases are complicated by atrial septal defects [3]. PAPVCs without atrial septal defects are relatively rare, as in our case. Specifically, one or more pulmonary veins failed to connect to the left atrium, resulting in a left-to-right shunt. The more the left-to-right shunt increases, the more severe the symptoms [4]. However, PAPVC may remain undiagnosed until adulthood because only a few clinical symptoms typically manifest [2]. Importantly, PAPVC is found in 0.1% of the adults examined using computed tomography [5]. Many reports have shown that older patients with PAPVC have an increased right ventricular strain and symptoms of right heart failure [2].
In the present case, we decided to perform a left lower lobectomy for radical resection. PAPVC was diagnosed incidentally during preoperative examinations.
A pulmonary-to-systemic flow ratio (Qp/Qs) of greater than 1.5 is one of the surgical indications of PAPVC [6]. However, the surgical indications for PAPVC have not yet been defined.
Blood from the PAPVC was perfused into the left brachiocephalic vein. Therefore, after lobectomy, we speculated that the hemodynamics would be similar to those found in left pneumonectomy due to blood flow from the PAPVC. We considered that the Qp/Qs increased and oxygenation decreased because the left-to-right shunt flow increased postoperatively.
Furthermore, we presumed that the patient had right heart overload because the preoperative transthoracic echocardiography showed right ventricular dilatation. ElBardissi et al. reported a patient who died of right heart failure due to uncorrected PAPVC after a lung cancer procedure [7]. Moreover, right-sided heart overload can cause right-sided heart failure in the long term. Therefore, we decided to correct the PAPVC.
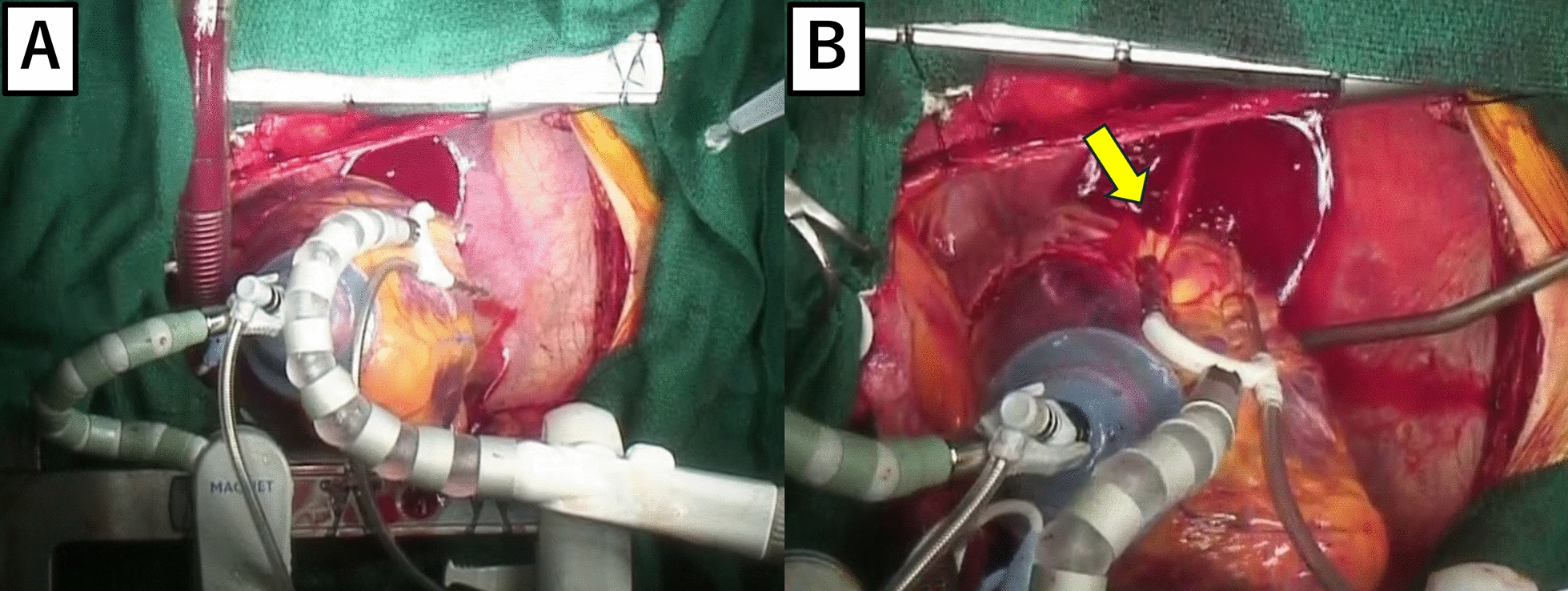
However, the operative procedure has not yet been established. Five cases of reconstructive PAPVC were associated with lung resection (Table 1) [8,9,10,11,12]. If the PAPVC was located in the same lung lobe to be resected, we identified an abnormal vessel and ligated it. Otherwise, careful measures should be taken. PAPVC on the right side necessitates intra-atrial flow diversion with cardiopulmonary bypass, employing techniques such as the Warden procedure or the double-decker method [3, 12]. In contrast, the left PAPVC could be reconstructed without cardiopulmonary bypass. In the present case, the PAPVC was anastomosed to the left atrial appendage for anatomical reasons. Takei et al. anastomosed an anomalous vein to the stump of a pulmonary vein connected to a resected lobe [8].
Table 1 Reconstructive cases of partial anomalous pulmonary vein connection associated with lung resectionPostoperatively, anticoagulation therapy was initiated to prevent thrombogenesis at the anastomotic site. The target prothrombin time-international normalized ratio was set at 2.0. Transthoracic echocardiography performed in the second postoperative month revealed no right ventricular overload. Therefore, warfarin was discontinued because the reconstructed vessel was not obstructed, and aspirin was continued.
The patient’s postoperative course was uneventful. This rare case of successful surgical treatment of PAPVC with lung cancer in different lobes can guide clinicians in managing similar cases.





留言 (0)