SFTs are a rare mesenchymal neoplasm of fibroblastic differentiation that can occur anywhere in the body. SFTs are composed of spindle-shaped cells that exhibit patternless growth and have both low- and high-density areas of cells. Many cases have been observed in collagenous backgrounds with staghorn-shaped blood vessels [3]. Considering immunohistochemistry, CD34 expression is a consistent finding; however, it can be positive in other types of soft tissue tumors. Leona et al. reported that nuclear expression of STAT6 was positive in almost all SFT cases and was limited to other soft tissue tumors. Strong STAT6 expression has high sensitivity and specificity as an immunohistochemical marker for SFT [4,5,6].
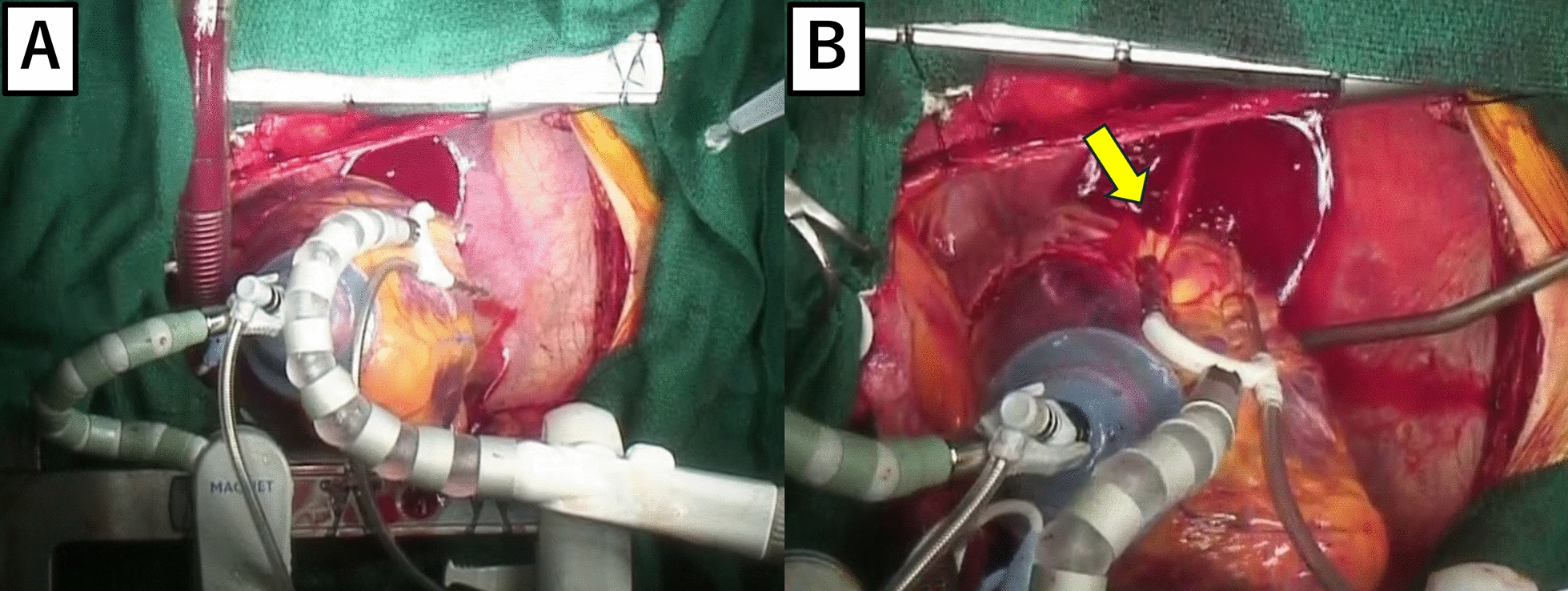
Since many tumors can have a similar growth pattern, the differential diagnosis is broad. Ostensibly, in cases with dedifferentiation the differential includes mostly malignant neoplasms. Owing to its affinity for the abdomen, gastrointestinal stromal tumor (GIST) should always be considered in the differential diagnosis of dedifferentiated SFT [7]. As with many soft tissue tumors, surgical resection is the standard therapeutic strategy for SFT. Most patients have a good prognosis after surgery, but extra-thoracic SFTs pose relatively higher risks for local recurrence than intrathoracic SFTs [8, 9]. Therefore, complete resection is necessary to reduce the risk of recurrence.
Demicco et al. analyzed 110 cases of SFT and established a 3-tier risk stratification model based on patient age, tumor size, and mitotic figures [10]. They reported that patients over 55 years old, with tumors greater than 15 cm, and mitotic counts greater than 4 mitoses/10 HPFs had the highest risk of metastases and mortality. Our case also showed typical pathological findings of SFT, including patternless growth of spindle cells, staghorn-shaped vessels, and strong nuclear expression of STAT6. There was no evidence of infiltrative growth, necrosis, dedifferentiation, or abnormal mitosis. The tumor had a maximum diameter of 7 cm, and mitotic counts 3 mitoses/10 HPFs. Therefore, the risk factor of our case was only the advanced age of the patient (70 years).
SFTs are rarely observed in the gallbladder, making their identification using preoperative imaging challenging. This complicates the decision-making process for the treatment strategy. When a malignant tumor is suspected in the gallbladder, cholecystectomy or extended cholecystectomy with or without choledochojejunostomy or hepaticojejunostomy is performed, depending on the situation. When it is difficult to make a preoperative diagnosis, pathological diagnosis during surgery is one strategy to avoid oversurgery. The accuracy of pathological diagnosis during surgery for gallbladder tumors is approximately 95% (97.0% for benign tumors and 94.7% for malignant tumors) [11]. From these data, we thought that it is acceptable to use pathological diagnosis as information for deciding the surgical strategy for gallbladder tumors; however, SFT originally have borderline malignant features; therefore, complex interpretations may be required. In fact, the diagnosis during surgery was mucinous carcinoma, although our patient showed typical pathological findings for SFT postoperatively. The background stroma of SFT sometimes shows focal or diffuse mucoid changes [12]. The intraoperative pathological findings show the pools of the mucinous component and variable amount of tumor cells (Fig. 5). Since the findings were already atypical for the gallbladder, they were deemed abnormal and raised suspicion for mucinous carcinoma. Considering the rarity of SFT originating in the gallbladder and the features of pathological findings, including background stroma, background mucoid changes may have influenced the intraoperative pathological diagnosis.
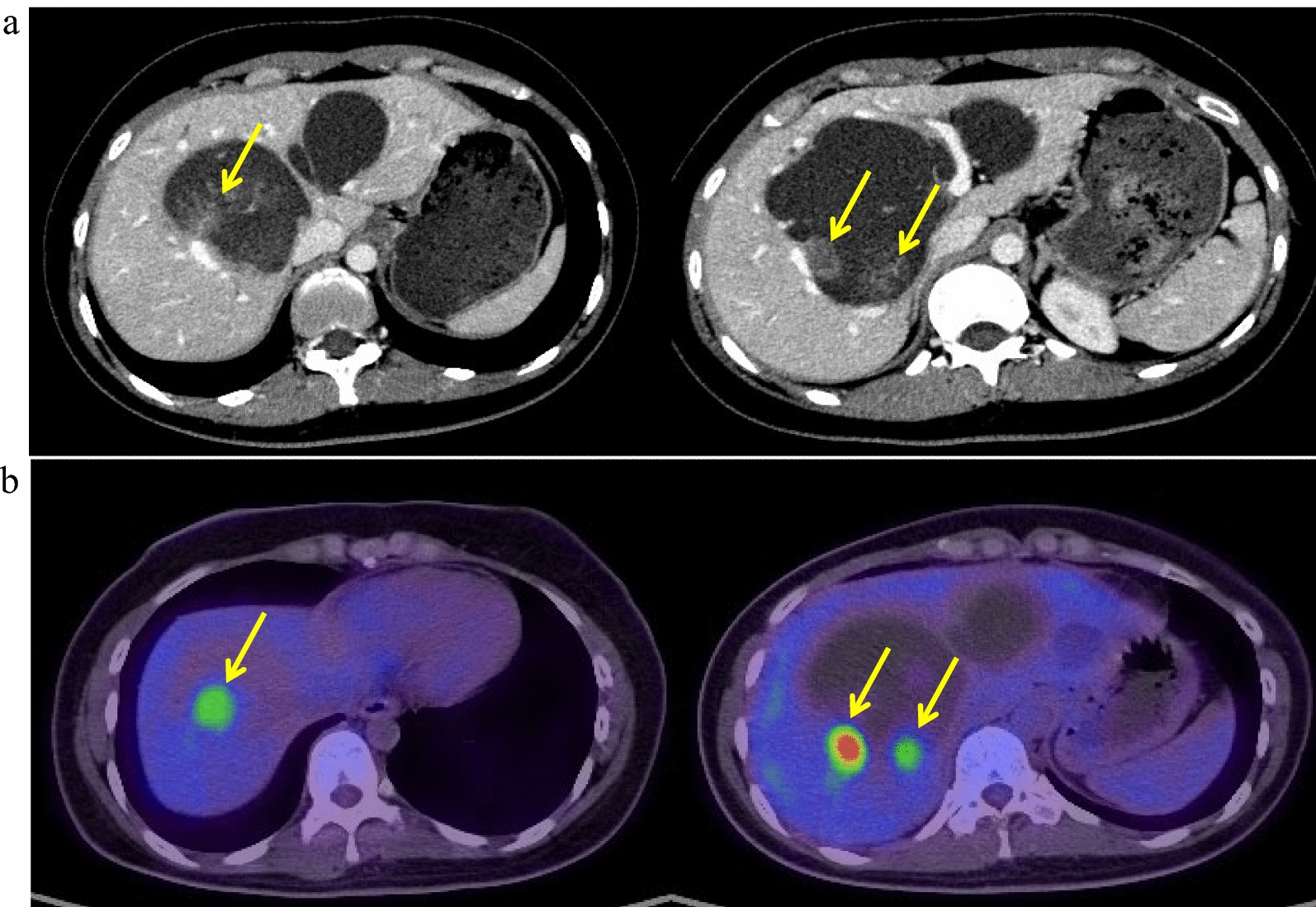
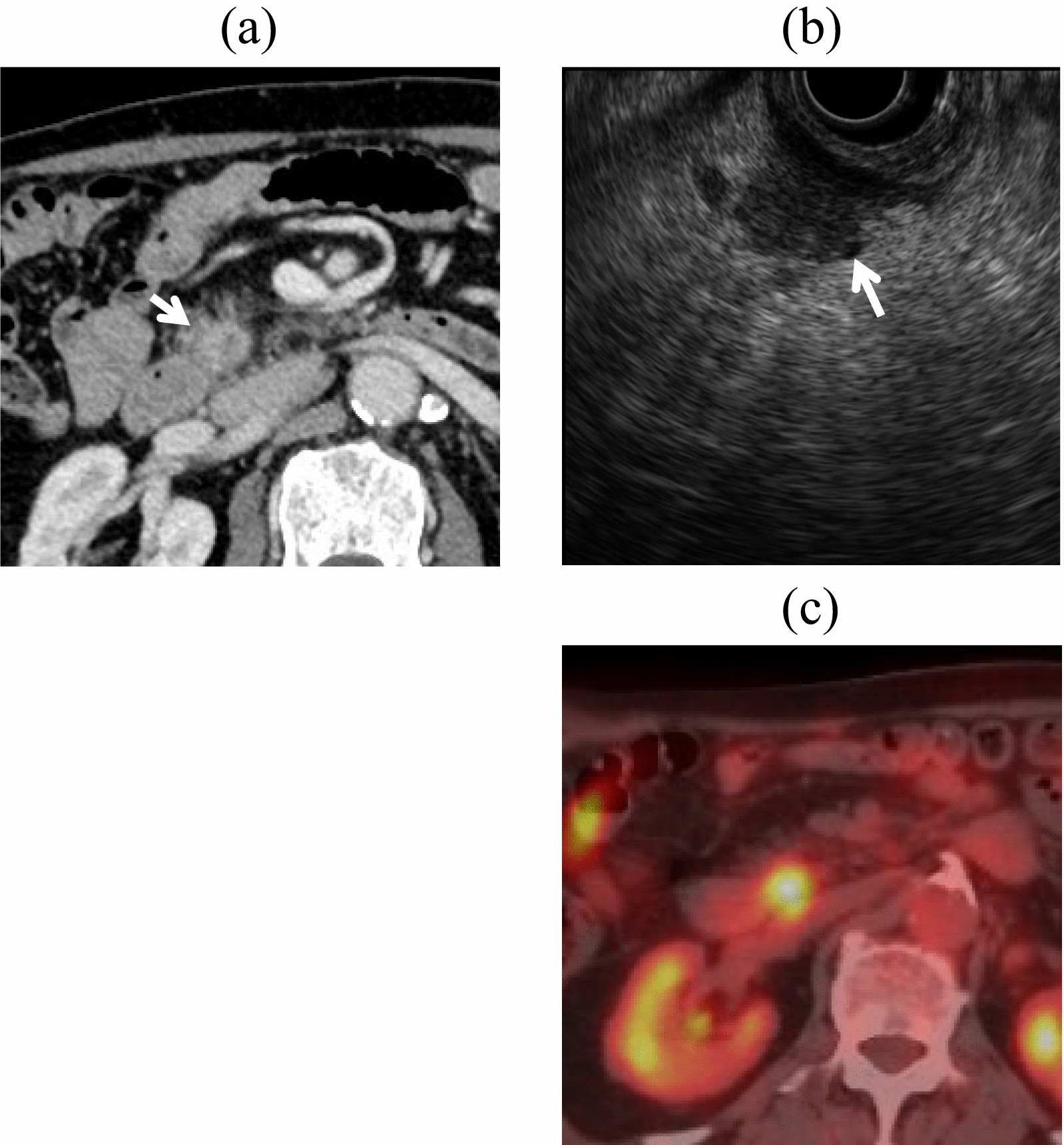
Ginat et al. reported the imaging features of SFT. On CT, an SFT appears as a clearly demarcated, sometimes lobulated, mass with contrast effects. In large tumors, cystic components, calcification, myxoid degeneration, and bleeding may be observed. On MRI, it usually shows low signals on T1- and T2-weighted images; however, if there are many cellular components or if there is edema, necrosis, or myxoid degeneration, it shows high signals on T2-weighted images [13]. In our case, CT revealed a contrast-enhanced mass with clear borders. MRI revealed a mass with a clear border that included hyperintense cystic and reticulated structures on T2-weighted images. Additionally, FDG-PET confirmed high-level FDG uptake in the gallbladder tumor in the early phase without increasing FDG uptake in the later phase. There are no reports on FDG-PET performed for SFTs; this finding may be helpful for imaging findings in future cases of SFTs.
Lazure et al. reported the first case of SFT of the gallbladder [2]. In their case, laparoscopic cholecystectomy was performed because of abdominal pain. Preoperative abdominal ultrasonography revealed cholelithiasis and thickening of the fundus of the gallbladder without a distinctive mass. Thus, the tumor was incidentally detected in the resected specimen. Therefore, this is the first report of an SFT of the gallbladder that was detected preoperatively.





留言 (0)