Implementing a colostrum-kit with the information and material needed for collecting the first colostrum from the birthing parent and transport to their infants admitted to the NICU, was significantly correlated with reduced time from birth to first received own colostrum (TOC) with a mean reduction of 29 h. The reduction in TOC was not only rapid and sustained over time after implementing the colostrum-kit, but TOC was subsequently decreasing through the periods of follow-up. Implementing new clinical routines takes time and the effectiveness of the implementation varies with how fast healthcare providers adapt to the new way of working. Therefore, is it not unusual to see a continuous increase in effectiveness after implementation if the belief in the importance of the routine is increasing [28]. The implementation of the kit in clinical care was preceded by information to the clinical staff about the kit and the importance of early initiation of lactation and administration of colostrum. The colostrum-kit serves a practical purpose, increasing the feasibility of early colostrum expression. Beyond its practicality, the routine also highlights the importance of early colostrum administration to the infant. Additionally, the kit was accompanied by a clarification of the healthcare workers responsibilities regarding supporting early colostrum expression. We believe that the continuous decrease in time to first colostrum might reflect an ongoing change in the attitudes of healthcare personnel regarding the importance of early colostrum. Future quality initiatives might supplant or overrun the effect of the colostrum-kit.
Several reports on interventions to increase the availability of own human milk in the NICU have been published, some of multimodal design and others with more isolated interventions. Both lactation rounds, lactation consults, and peer supporters have shown positive effects, as well as kangaroo mother care and early provision of colostrum [19]. Implementing an extensive multimodal quality-improvement programme requires funding and resources for design, implementation and evaluation, and the effect is usually quite limited. The colostrum-kit is on the other hand a low-cost intervention, consisting of material already available and in use, taking an assistant nurse about an hour per week to prepare for a unit with approximately 950 NICU-submissions/year while saving the midwives’ time.
Fleiss et al. performed a quality-improvement study with multimodal design, optimising the knowledge and routines among NICU-staff on early colostrum, increasing the proportion of very low birthweight infants receiving colostrum within 6 h, from 6% (N = 70) to 55% (N = 37) [22]. When analysing our data in a similar birthweight-cohort results were G0: 6% (N = 158), G1: 26% (N = 164), G2: 38% (N = 163) and G3: 52% (N = 151), and thereby reaching the same effect but with probably a more low-cost intervention. In 2018 Kristensen-Cabrera et al. presented a prospective study on a dedicated colostrum collection system for electric breast pumps [29]. The results showed that Primo-Lacto did help facilitate successful colostrum collection. An advantage with the Primo-Lacto is that the system is closed, reducing the risk for contamination, but the cost is higher, and the availability is lower compared to the colostrum kit presented in this study.
Subgroup effects
The reduction in Time to first Own Colostrum was significant in all subgroups of gestational ages and mode of delivery with a larger reduction in TOC in the group of lowest gestational age and the group delivered by caesarean section. Earlier studies have implied that initiating lactation after very preterm birth and/or caesarean section is complicated due to physiological factors delaying lactogenesis [30]. Murase et al. showed a strong association between caesarean section and delayed initiation of milk expression [14]. Our results showed a large difference in TOC between groups of GA or mode of delivery in the pre-implementation cohort. This disparity corresponds to the belief that parents delivering very preterm or by caesarean section struggles with expressing colostrum. However, after implementation, the difference between these subgroups disappeared. This could indicate that the physiological component for how early after birth it is feasible to express colostrum, is smaller than the component of information and support. It is common for healthcare providers to be cautious about informing and encouraging birthing parents to express colostrum close after giving birth to an infant that needs critical care, even though they are aware of the benefits of own human milk [31]. On the other hand, research shows that families depend on getting early information to be able to make informed decisions about early provision of colostrum, and that the information is effective regardless of socioeconomic background [32]. The nature of the colostrum-kit being easy-accessed and low-effort to distribute to all families promotes a high compliance to the routine, regardless of health staff work-load. The concept of a standardized and clear routine might also bridge the hesitation and cautiousness of many healthcare professionals, making it easier to deliver information in a neutral way, thus increasing the compliance further.
Implication for clinical care and future studies
There is a need for further studying the effect of early oropharyngeal colostrum since the studies that have been conducted to this date have shown varied results. In the Cochrane report on the subject, the definition of “early colostrum” was set to < 48 h [15], which is quite late regarding the WHO recommendations for immediate expression, and oral administering of colostrum to the sick or preterm infant unable to suckle after birth [7], especially in regard to early nosocomial infections. Our study shows that it is feasible to drastically reduce the time to first colostrum at a low cost, making it possible to conduct studies with narrower definitions on early colostrum that might have an increased chance to produce significant results.
Furthermore, the colostrum-kit has a potential to reduce disparity due to the possibility to have the written information in several languages, with complementing audio–video-instructions and pictograms making the information accessible for different needs and learning-types.
Strength and limitations
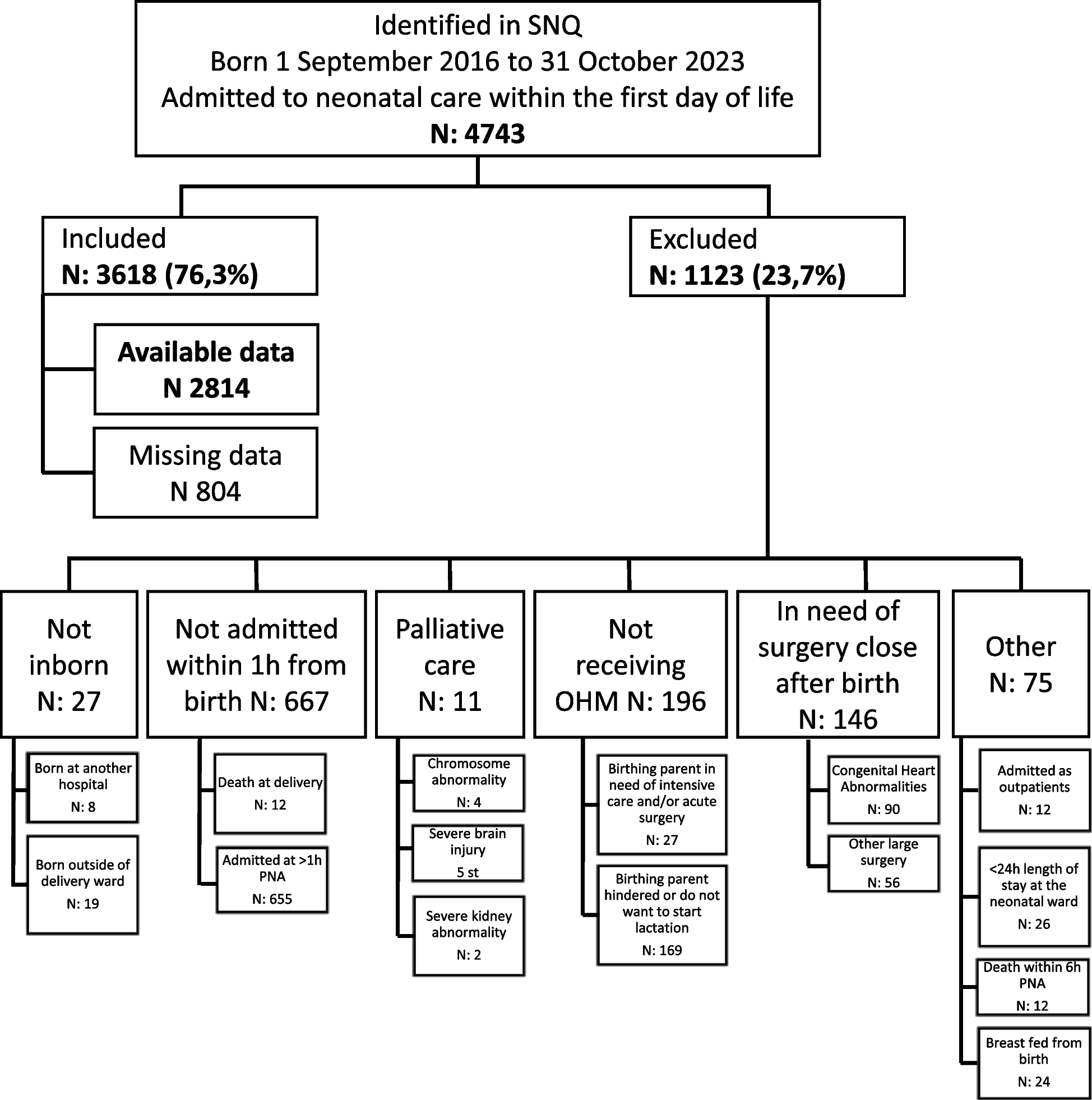
A major strength of this study is the large number of participants with close to 100% participation in the SNQ-register. Confounding variables for the provision of OHM such as GA, mode of delivery and insulin treatment during pregnancy, were available for all participants and comparable between groups. Another strength is the long follow-up of 5 years post implementation showing a persistent reduction in Time to first Own Colostrum.
The single-centre design and a large number of missing observations among term infants are limitations that need to be considered when interpreting the results. However, compared to the other five university hospitals, the study centre had a higher proportion of infants with available TOC data than other centres. In 2022 there were available data for 71% of admitted preterm infants and 39% of term infants at the study centre, compared to 44% and 19% of preterm and term infants respectively admitted to the other five university hospitals combined. The proportion of missing data is higher among term infants, but at the same time the length of stay is significantly shorter among infants with missing data. This could reflect a staff attitude not viewing early colostrum as essential for term infants or when the length of stay is expected to be short. The differences in available data affects the transferability of results regarding term infants with a short length of stay. Additionally, the implemented colostrum-kit only included information in Swedish, limiting the availability for non-Swedish speaking parents.






留言 (0)