Study design, setting, and population
The Fatty Liver Disease after Gestational Diabetes Mellitus (FLD-GDM) study was an umbrella project exploring various aspects of hepatic steatosis in women with a history of GDM. Conducted between November 2021 and February 2024 at a university hospital in Bangkok, Thailand, the study followed women for approximately 1 year postpartum after a GDM pregnancy. It served as a prospective observational extension of earlier research on breastfeeding and postpartum weight changes and their effects on metabolic health at 6 months postpartum [15, 19].
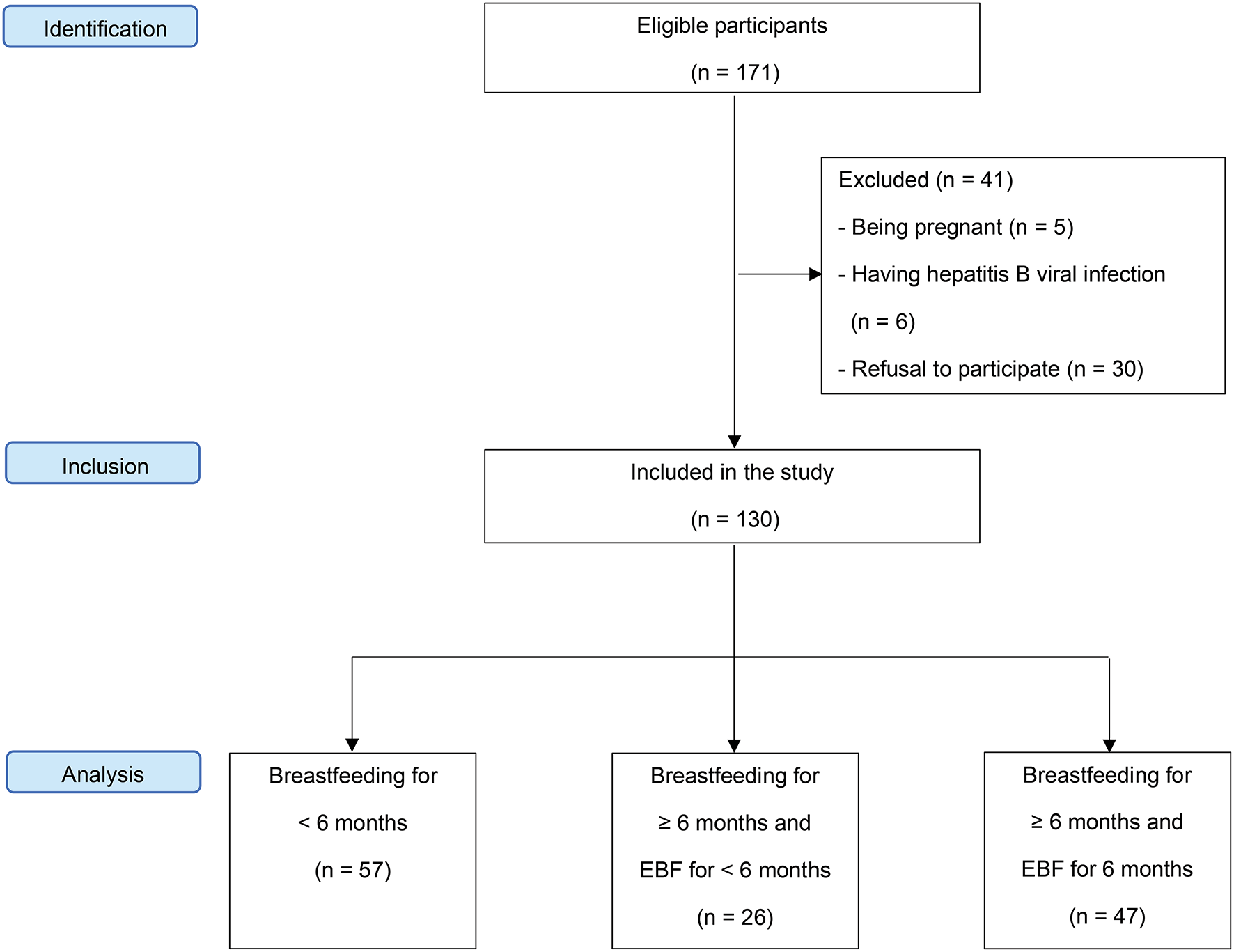
This sub-project of the FLD-GDM study specifically examined the relationship between breastfeeding, liver fat accumulation, and NAFLD prevalence. The study protocol was approved by the Institutional Review Board (certificate no. 117/2564) and adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Participants were required to have been part of earlier studies on breastfeeding and postpartum weight changes [15, 19]. The exclusion criteria included current pregnancy, alcohol consumption, hepatitis B or C viral infections, receiving medications associated with hepatic steatosis, such as corticosteroids, amiodarone, valproate, tamoxifen, and methotrexate, and refusal to participate.
For earlier studies, the inclusion criteria were: (1) age ≥ 18 years; (2) having antenatal care and GDM screening at the hospital; and (3) being diagnosed with GDM based on the Carpenter and Coustan criteria [20]. Exclusion criteria included HIV infection, pregnancy during the study period, use of contraindicated medications during breastfeeding, and loss during follow-up.
Sample size
The sample size was calculated based on findings from a previous study indicating a 62.7% prevalence of NAFLD in women with a history of GDM [7]. To detect a 54% reduction in NAFLD prevalence among women who breastfed for ≥ 6 months [16] (from 62.7 to 28.8%) with 80% power at a two-sided significance level of 0.05, a minimum of 99 participants was required. These participants were divided into three groups: 33 women who breastfed for < 6 months, 33 who breastfed for ≥ 6 months and exclusively breastfed for < 6 months, and 33 who breastfed for ≥ 6 months and exclusively breastfed for 6 months. This study is a prospective observational extension of previous studies that examined the effects of breastfeeding and postpartum weight changes on metabolic health at 6 months postpartum in women with prior GDM [15, 19]. Consequently, the present study included all women who participated in these earlier studies.
Participant recruitment
Potential participants were approached when presenting for follow-up 6 months postpartum in earlier studies [15, 19] or while attending the gynecology outpatient clinic for an annual Pap test 1 year after delivery. Participants were informed about the FLD-GDM study. All participants provided written informed consent before participating in the study.
Eligible participants were scheduled for blood tests and liver fat quantification at approximately 1 year postpartum, within a time frame of 15 months after delivery. They were instructed to refrain from eating or drinking anything 12 h before their scheduled appointment.
Procedure
On the scheduled date, participants were interviewed about their breastfeeding practices. They were asked about the duration of breastfeeding, the time at which they stopped breastfeeding or expressed milk, and the time they introduced formula or foods/drinks. Furthermore, feeding practice data were obtained from records in a mini calendar provided to the participants and the hospital’s electronic database during the baby’s routine follow-up visits [15]. A specially trained nurse performed a physical examination, measuring height, weight, blood pressure, and waist circumference (WC), as detailed in a previous publication [19].
After the physical examination, venous blood samples were drawn for fasting plasma glucose (FPG), glycated hemoglobin (hemoglobin A1c), insulin, and C-peptide; lipid analyses including cholesterol, triglycerides (TG), low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol (HDL-C); and liver function tests including aspartate aminotransferase, alanine transaminase, and alkaline phosphatase. All blood samples were collected after a 12-h overnight fast. FPG, hemoglobin A1c, and lipid measurements were performed using standard techniques as previously described [19]. Fasting insulin and C-peptide levels were analyzed with a Cobas e801 (Roche Diagnostics, Mannheim, Germany). Liver function tests were performed using a Cobas c503 analyzer (Roche Diagnostics). The homeostasis model assessment of insulin resistance was calculated using the following formula: fasting glucose (mg/dL) x fasting insulin (µU/mL) / 405 [21]. Prediabetes was defined as FPG ≥ 100 mg/dL [22], and MetS was diagnosed following the joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention [23].
Liver fat was measured using the controlled attenuation parameter (CAP) via the transient elastography model FibroScanⓇ 502 Touch (Echosens, Paris, France), with liver stiffness measurements (LSMs) conducted simultaneously. All examinations were performed by a single experienced hepatologist blinded to participants’ clinical data, using either a 3.5 MHz M probe or a 2.5 MHz XL probe, depending on the participant. Measurements were taken on the right lobe of the liver through the intercostal spaces, with the participants lying supine with the right arm in abduction. The success rate was calculated as the number of successful measurements divided by the total number of measurements. The median values of successful CAP and LSM measurements were reported in decibels per meter (dB/m) and kilopascal (kPa), respectively. Reliable measurements required ≥ 10 valid measurements, a success rate of ≥ 60%, a CAP interquartile range (IQR) < 40 dB/m, and an LSM IQR/median ratio < 0.3. Only measurements meeting these criteria were included in the analysis.
Data collection and outcome measures
Data collection included baseline characteristics at 6 weeks postpartum and clinical data at approximately 1 year after delivery. Baseline characteristics were drawn from earlier studies [15, 19], while 1-year data included breastfeeding practices, contraception methods, body mass index (BMI), blood pressure, WC, laboratory results, CAP value, LSM, and NAFLD status. Due to the lack of a standardized CAP threshold for detecting steatosis in this population, we used a cutoff of 302 dB/m, as identified in a prior study on adults suspected of NAFLD [24].
The participants were divided into three groups based on the duration and intensity of the breastfeeding: group 1 (breastfeeding for < 6 months), group 2 (breastfeeding for ≥ 6 months and EBF for < 6 months), and group 3 (breastfeeding for ≥ 6 months and EBF for 6 months). EBF was defined as feeding only breast milk without additional foods or liquids [25], with the duration assessed from birth to six months postpartum. The outcome measures were liver fat content and NAFLD prevalence.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 28.0 (IBM Corporation, Armonk, NY, USA). Chi-squared or Fisher’s exact tests, as appropriate, were performed to compare categorical variables. The means of continuous variables between the three breastfeeding practice groups were compared using a one-way analysis of variance. When the overall comparison showed significant differences, intergroup comparisons were performed using the least significant difference method as a post hoc test. Differences in the medians of continuous variables among the three groups were analyzed using the Kruskal–Wallis H test, followed by the Dunn-Bonferroni post hoc test for pairwise comparisons.
Changes in the means of variables over time (between baseline and 1 year postpartum) within each group were analyzed using paired t-tests. Differences in these changes between the three groups were examined using a one-way analysis of covariance, controlling for the baseline value of each parameter. Changes in the prevalence rates of prediabetes and MetS within each group over time were calculated using McNemar’s test, while differences in these changes between the three groups were compared using the chi-squared test. To assess the relationship between breastfeeding and NAFLD, multivariate logistic regression analysis was performed after adjusting for an a priori set of confounding variables: age, severity of GDM, method of contraception used, baseline BMI, and FPG [16, 17, 26]. Adjusted odds ratios (ORs) were estimated with 95% confidence intervals (CIs). All tests were two-sided and statistical significance was set at p < 0.05.






留言 (0)