Study design and population
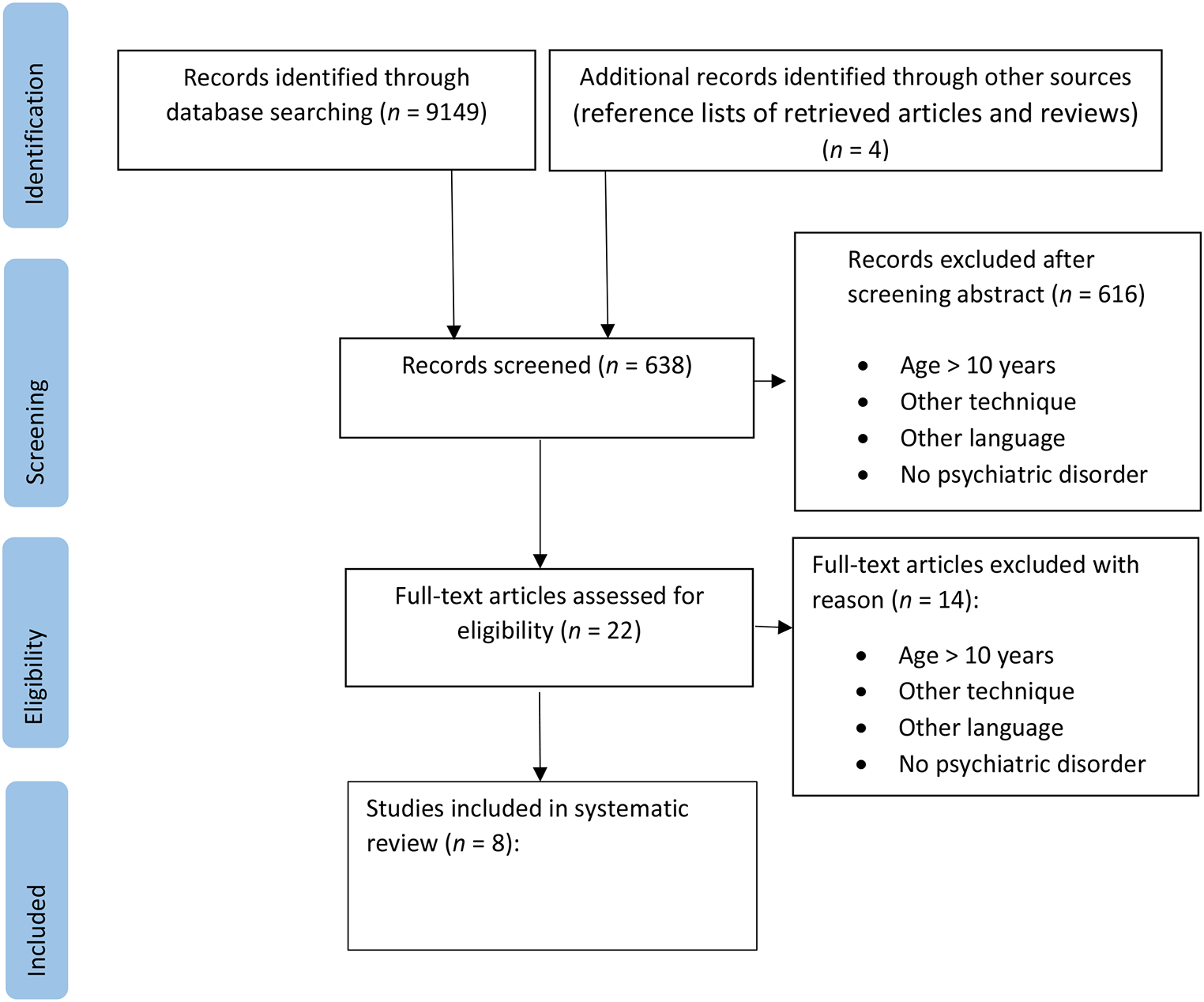
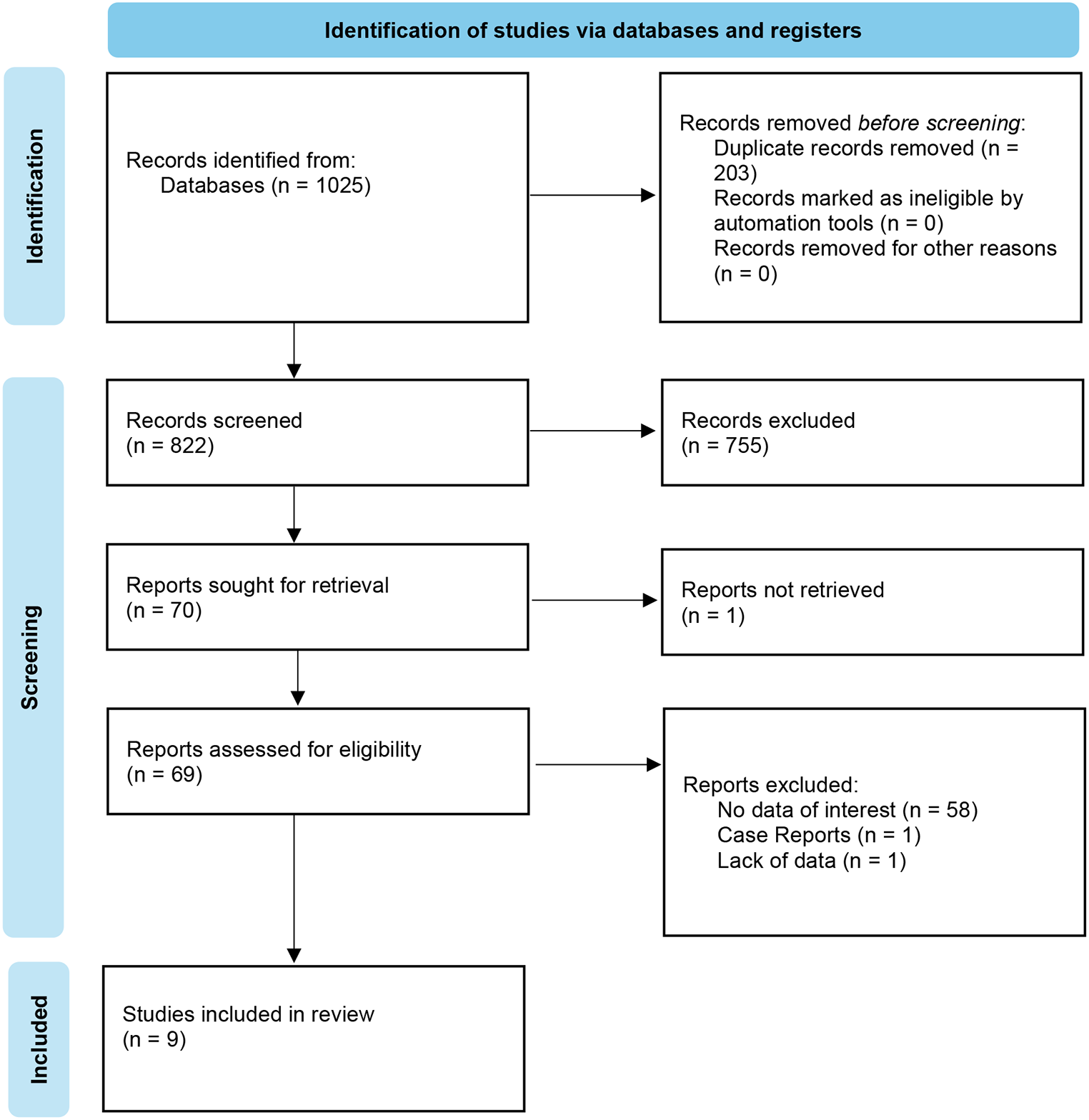
The study population were based on participants in the Danish National Birth Cohort (DNBC). The DNBC is a nested sub-set of the entire population of Danes born during mid-1996 to mid-2003 (N = 451,768). Pregnant women were invited to participate in DNBC through their general practitioner (GP) during these years with intentions of terminating pregnancy and insufficient language skills as the only exclusion criteria [11]. Approximately 100,000 pregnancies were enrolled resulting in 96,822 liveborn children [11]. Between 2016 and 2021, when the participants turned 18 years and three months, they received an online questionnaire (DNBC-18). Out of 43,771 eligible girls and 45,434 eligible boys, 27,723 girls (63%) and 20,129 (44%) boys (total: N = 47,852, 54%), respectively completed the questionnaire up until the suicidality items (Figure S1, available online). The questionnaire was designed with mandatory responses and if quit early, the completed responses were retained, while unanswered items would be missing. Thus, 26,131 girls (60%) and 18,448 (41%) boys (in total: N = 44,579, 50%), completed all indicators of mental health and well-being, risk behaviors, and social life factors used in this study. These two samples (N = 47,852 / N = 44,579) constituted the central study populations. Data on suicide plans was only available for participants who completed the DNBC-18 after May 2019. Thus, only sub-populations of the former groups (N = 19,182 / N = 17,829) were available for this form of suicidality. All individuals living in Denmark are issued with a unique personal ID number [12]. This enabled us to link data from the DNBC with register data on hospital-recorded suicide attempt (Table S1).
MeasuresSuicidality
Information on self-reported suicidality was obtained from DNBC-18 (Table S2). Participants could answer ‘yes’, ‘no’ and ‘do not know’, when asked whether they ever had experienced suicidal ideation, i.e., “Have you ever thought about taking your own life (even though you would not do it)?”, plans, i.e., “Have you ever had suicide plans (considered methods, done preparations)?”and attempts, i.e., “Have you ever tried to take your own life?”. Questions in DNBC-18, which were perceived as particularly sensitive, included ‘do not know’ as a response option. Respectively, 4%, 3%, and 1% of participants replied ‘do not know’ to items regarding suicide ideation, plans and attempts. These were categorized as ‘no’ replies. Participants who responded affirmatively to questions regarding suicide ideation or attempt were also asked about frequency of these events within the last year. These questions were used to assess whether participants recently had experienced suicidality.
Information on hospital-recorded suicide attempts were retrieved from the National Patient Register including both inpatient, outpatient, and emergency room contacts [13]. Suicide attempt was defined as (a) a diagnosis of deliberate self-harm recorded according to the International Classification of Diseases, version 10 (ICD-10) as X60-X84 or where suicide attempt was recorded as the reason for contact. Suicide attempts are under-recorded in Danish hospital settings and we therefore include other contacts, which were likely to be suicide attempts [14]. These were identified as (b) intoxication with specific drugs, (c) a psychiatric diagnosis in combination with intoxication with all drugs and biological substances except alcohol, or d) a psychiatric diagnosis in combination with injuries to the lower forearm (Table S2). This algorithm has previously been applied [15,16,17]. We only included records of individuals aged 10 years or older as suicide attempts registered in younger individuals could be more likely to reflect accidents or registration error [15]. The admission date in the record was used to determine whether the suicide attempt occurred within a year prior to the completion date of DNBC-18.
A composite measure of form of suicidality was formed with the following mutually exclusive categories: no suicidality, self-reported suicide ideation, self-reported suicide attempt, and hospital-recorded suicide attempt. Participant were classified according to their most severe form of suicidality [5]. When analyzing data from the sub-population where information on suicide plans was available, the mutually exclusive categories were: no suicidality, self-reported suicide ideation, self-reported suicide plans, and suicide attempt (self-reported or hospital recorded). Further, an additional measure with the following mutually exclusive categories was constructed to compare adolescents who never, previously, and currently had any form of suicidality: no suicidality, past suicidality (> 1 year prior to completing DNBC-18), and current suicidality (≤ 1 year before completing DNBC-18).
Factors on poor mental health and well-being, risk behavior and social life factors
Measures of poor mental health and well-being consisted of depressive symptoms [18], poor mental well-being [19,20,21], self-injury within the past year, disordered eating behavior symptoms [22], social anxiety symptoms [23], panic anxiety symptoms [23], externalizing problems [24,25,26], internalizing problems [24,25,26], low quality of life [27, 28], and self-assessed health (Table S3). Measures of risk behavior reflected the adolescents willingness to engage in activities or behaviors, which potentially could lead to morbidity, mortality, or other negative consequences [29]. These included alcohol dependence [30, 31], daily smoking, tried cannabis within the last year, tried other drugs within the last year, and sleep deficiency (< 7 h/night) [32]. Social life factors comprised whether adolescents engaged in supportive social relations or had experiences of loneliness, difficulties making friends, and low social abilities [24,25,26].
Statistical analyses
All data management and statistical analyses were conducted in SAS version 9.4. Sample weights were calculated based on inverse probability weighting (IPW), using peers from the general population i.e., all Danes born during the same years as DNBC children alive at age 18 years (N = 449,288). By allocating larger weight to individuals with a lower probability of participating in DNBC-18, we were able to compensate for differential participation and attrition [33]. In a logistic regression model, we estimated probability of participating in DNBC-18 based on highest parental education, parental income, parental job-status, maternal age at birth, parity, co-living parents, out-of-home placement, any childhood or adolescent psychiatric diagnosis, and any history of parental psychiatric diagnosis (Table 1). All variables were derived from Danish registers and were linked using the unique personal ID number assigned to all residents (Table S1). Weights were calculated separately for boys and girls and truncated to the cut-off value of median + 5*IQR and used in subsequent analyses [34].
In the main analyses, all factors of poor mental health and well-being, risk behavior and social life factors were examined as binary variables. Characteristics based on scales were dichotomized according to previous literature [18, 21, 22, 25,26,27,28, 31]. Weighted proportions were calculated for adolescents with no suicidality, self-reported suicide ideation, plans and attempts, and hospital-recorded suicide attempt with their corresponding 95% confidence intervals (95% CI). Similarly, weighted proportions were calculated for no, past, and current suicidality. P-values based on chi-square tests were used to compare: (1) no suicidality vs. suicidal ideation, (2) suicidal ideation vs. self-reported suicide attempt, and (3) self-reported suicide attempt vs. hospital recorded suicide attempt. Similar tests were performed for the sub-group analyses. All analyses were stratified by sex.
Sensitivity analyses
In sensitivity analyses, measures based on scales were examined as continuous variables and presented as weighted mean scores with corresponding 95% CI for each form of suicidality. P-values based on t-test were used to compare suicidality groups as described in the main analyses. Adolescents replying ‘do not know’ to suicidality might differ from those replying ‘no’. Therefore, we conducted a sensitivity analysis where participants replying ‘do not know’ were categorized as a separate group.
Table 1 Characteristics of the general population of children born in mid-1996 to mid-2003 and participants in the 18-year follow-up of the Danish National Birth Cohort (DNBC-18) born during the same period with and without applied sample weights 



留言 (0)