
記住我





The study cohort consisted of 447 consecutive AML patients treated at the Clinical Division of Hematology, Med Uni Graz, Austria. In more detail, we included the data from 284 patients treated in the NGS era (2013–2023) and 163 patients treated before this time (2002–2008). Detailed clinical characteristics are depicted in Supplementary Tables 1 and 2.
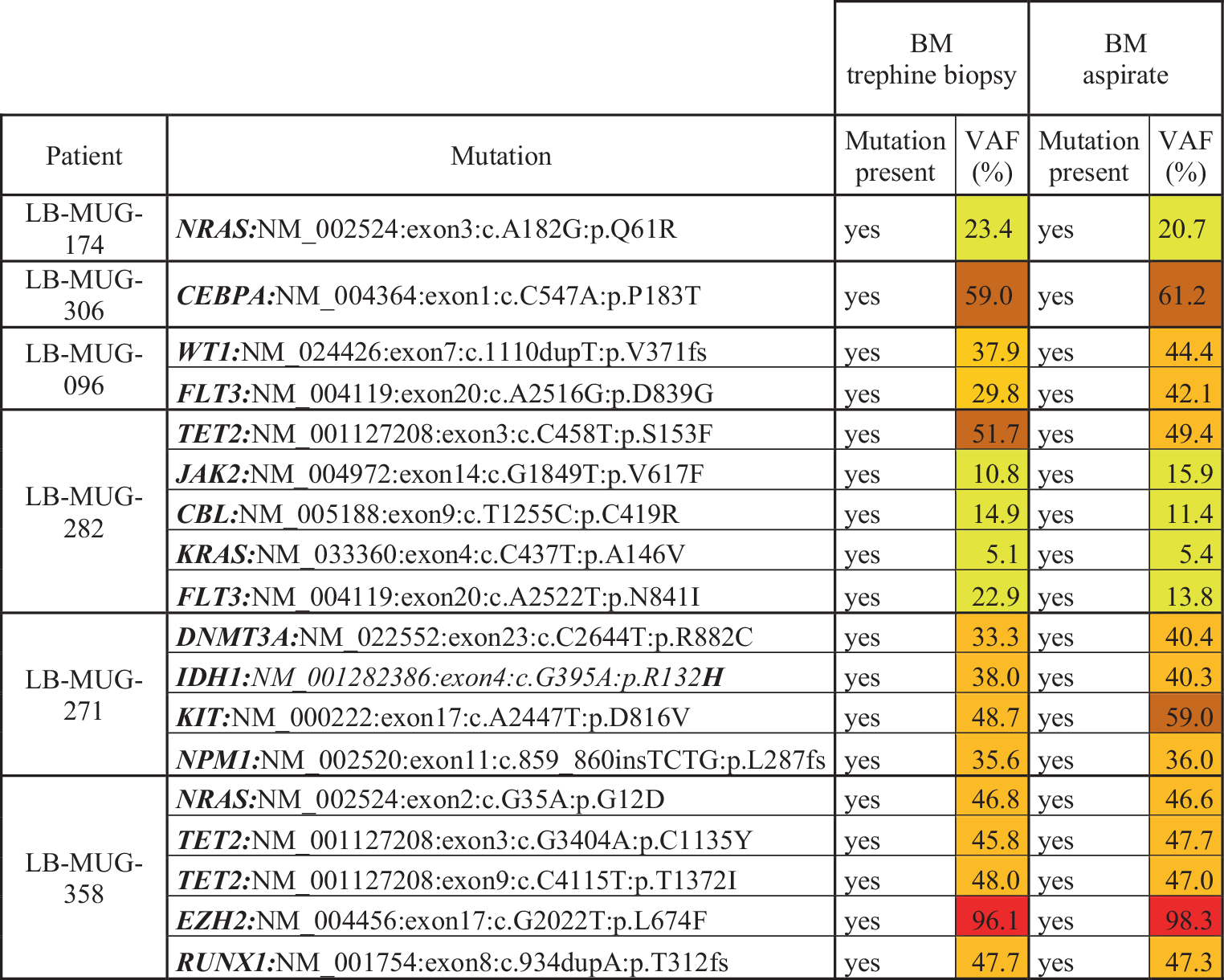
Application and results of NGSA focus of this study was to evaluate the applicability and outcomes of NGS profiling within a routine clinical setting. The NGS has been available for the routine work-up of AML at the Institute of Pathology, Med Uni Graz since 2013. It was ordered by the treating hematologist in 267/284 (94%) of patients. The cases where no NGS was ordered were predominantly patients treated with hypomethylating agents (HMA) or best supportive care (BSC) only, but also three individuals treated by intensive chemotherapy (ICT) diagnosed before 2016. While we primarily aimed for NGS analyses from BM aspirates, this procedure was not possible in all patients at diagnosis, i.e., in case of dry tabs. Therefore, we performed comparative experiments, analyzed BM trephine biopsies and corresponding aspirates from six patients, and observed comparable results (Fig. 1).
Fig. 1
Comparison of NGS results from BM trephine biopsies and aspirates. For better visibility and comparability between BM trephine biopsies and aspirates, VAF < 25% are highlighted in yellow, VAF ≥ 25% and < 50% in light orange, VAF ≥ 50% and < 75% in dark orange, and VAF ≥ 75% in red. NGS next-generation sequencing, LB-MUG Leukemia Biobank Med Uni Graz, BM bone marrow, VAF variant allele frequency
Consequently, we routinely performed NGS from trephine biopsies in case of missing or insufficient aspirates. This led to successful NGS analyses in all patients allocated for sequencing at the Med Uni Graz between 2013–2023 included in this study. As a comparison, the combination of cytogenetic analyses and targeted Fluorescence In Situ Hybridization (FISH) markers was attempted in all patients but yielded an evaluable result less frequently (259/284 cases, 91%, P < 0.0001). The reasons behind this were either dry tap bone marrow aspirations or missing growth of cells that did not allow G‑banding. Of importance for the routine clinical setting, 10 patients with missing cytogenetics could still be risk-stratified, according to ELN2022, using molecular NGS techniques from the BM. This increased diagnostic accuracy is due to the detection of mutated TP53 in sequencing and the identification of prognostically determining translocations in NGS-based RNA translocation analyses, as described by our group previously [7]. We then assessed the duration from BM sampling until the availability of NGS results. The average time for this period was 16 days, with decreasing values from 2013/2014 (22 days) to 2022 (10 days). Of note, the average time from BM sampling until the availability of cytogenetic results was comparable to NGS (18 days) with decreasing values from 2013/2014 (26 days) to 2022 (11 days). Another important aspect of NGS usefulness in the clinical routine is its potential to identify targetable molecular lesions. Currently, these include mutations in FLT3, IDH1 and IDH2, where drugs licensed by the European Medicines Agency (EMA) and/or the U.S. Food and Drug Administration (FDA) are available. Altogether, within our cohort, NGS identified mutations within these genes in 107/284 (38%) of patients, further supporting its relevance for the routine clinical management of AML.
Concerning the molecular profile observed, we corroborated previously published mutational landscapes of AML (Fig. 2). The most frequently mutated genes included TET2 (n = 73/267, 27%), FLT3 (n = 66/267, 25%), DNMT3A (n = 60/267, 23%, and NPM1 (n = 60/267, 23%) [22,23,24,25]. Importantly, our study also includes NGS data from older patients treated with nonintensive chemotherapy (NICT) or BSC only. Therefore, our data reflect a real-world perspective of AML, not biased by the potential inclusion criteria of CCITs. When comparing older patients ≥ 70 years (median 77 years, range 70–88 years) with younger patients < 70 years (median 59 years, range 19–69 years), we found an enrichment of mutations in IDH2, SRSF2, TET2, and TP53 in the older patient cohort (IDH2: 18/81, 22% in older patients vs. 16/186, 9% in younger patients P = 0.004; SRSF2: 15/81, 19% in older patients vs. 9/186, 5% in younger patients P < 0.001; TET2: 31/81, 38% in older patients vs. 42/186, 23% in younger patients P = 0.011; TP53: 21/81, 26% in older patients vs. 28/186, 15% in younger patients P = 0.040). With respect to mutation categories, we observed an increased frequency of mutations affecting DNA methylation and the spliceosome in the older patients (DNA methylation DNMT3A, TET2, IDH1/2: 58/81, 72% in older patients vs. 84/186, 45% in younger patients P < 0.001; spliceosome SRSF2, ZRSR2, U2AF1, SF3B1, SF3B2: 23/81, 28% in older patients vs. 21/186, 11% in younger patients P = 0.006). On the contrary, mutations affecting cellular signalling were more frequent in younger patients (FLT3, NRAS, KRAS, KIT, CBL, PTPN11, BRAF, CALR, CSF3R, JAK 2, NF1; 37/81, 46% in older patients vs. 114/186, 61% in younger patients P = 0.022). We also observed enrichment of MDS-related mutations according to the World Health Organization (WHO) 2022 classification [26] in older patients (33/81, 41% in older patients vs. 48/186, 26% in younger patients P = 0.020). The NGS distribution data and mutation heatmaps of older and younger patients are presented in Table 1 and Supplementary Figures 2–3.
Fig. 2
Molecular landscape of 267 AML patients analyzed with NGS. a Mutation frequencies. b Oncoplot showing nonsynonymous mutations in individual genes, grouped into categories, as labeled on the left. Every column on the x-axis represents a single patient. Colors reflect the ELN2022 risk groups. Only genes with at least one mutation are shown
Table 1 Mutation frequencies in older and younger AML patientsProgress in AML treatment over timeIn the next step, we were interested in whether the outcome of AML patients improved in the NGS era. Therefore, we compared treatment outcomes to a cohort of 163 unselected, consecutive patients treated between 2002–2008 at our division. Of note, neither NGS nor molecularly targeted therapies were available at this time. Except for low-dose Ara‑C (LDAC), non-intensive AML treatment options were also not available. Therefore, for better comparison, we focused our analyses only on intensively treated patients receiving 7 + 3 based regimens ± allogeneic hematopoietic stem cell transplantation (allo-HSCT) and compared 167 patients treated between 2013–2023 with 163 cases treated between 2002–2008. We first compared overall survival (OS) and observed a significant elongation in patients treated between 2013–2023 (median survival 910 days for 2013–2023 vs. 371 days for 2002–2008; P = 0.002; Fig. 3a) with a hazard ratio (HR) of 0.65 (95% confidence interval, CI 0.49–0.86). When searching for potential reasons behind improved OS in the 2013–2023 cohort, descriptive statistics revealed an increased rate of allografting and a higher rate of complete remissions (CR)/CR with incomplete count recovery (CRi) to first line therapy within these patients, while all other factors assessed (age, sex, white blood cell count, WBC, peripheral blood, PB, blasts and lactate dehydrogenase, LDH) were similarly distributed between the groups (Supplementary Table 2). Importantly, allo-HSCT and CR/CRi to first line therapy were associated with prolonged survival in univariable analyses and remained independent significant factors in multivariable models (Supplementary Table 3). Hence, these data suggest that the better survival in the 2013–2023 cohort is mainly mediated through a higher transplantation frequency and a better treatment response to first line regimens. Interestingly, the median age at transplantation was also higher in the 2013–2023 cohort (2002–2008: median 46 years, range 18–68 years; 2013–2023: median 56 years, range 19–71 years; P < 0.001), reflecting the clinical experience that allo-HSCT is more often offered to older patients nowadays. We did not have sufficient information on the cytogenetic analyses in the 2002–2008 cohort, precluding comparison of specific karyotype-defined risk groups between the 2002–2008 and 2013–2023 cohorts.
Fig. 3
Comparison between the NGS-era (2013–2023) and the pre-NGS era (2002–2008). a Comparison of overall survival between patients treated with intensive chemotherapy (ICT). b Cumulative CR/CRi rates in patients treated with ICT between 2002–2008 and 2013–2023. Results of multivariable analyses are displayed in Supplementary Table 3
Progress in AML treatmentOur data reveal increased use of allo-HSCT and higher rates of CR/CRi after first line therapy as major determinants of improved survival in recent times. Considering higher response rates to first line therapy, it could be hypothesized that this is caused by the advent of novel and molecularly targeted drugs that can be applied after NGS-based molecular characterization. To elaborate on this topic, we performed exploratory analyses studying potential effects of selected novel substances in the 2013–2023 cohort.
Midostaurin is a FLT3 inhibitor and is nowadays added to 7 + 3-based ICT in FLT3 mutated AML patients [8]. It was licensed by the EMA in 2017; therefore, the 2013–2023 cohort comprises FLT3-mutated patients treated with and without the addition of midostaurin (n = 13 patients ICT + midostaurin vs. 38 patients ICT only). When comparing the OS between these groups, patients treated with ICT and adding midostaurin had a significantly better survival (median survival 427 days for ICT vs. median survival not reached for ICT + midostaurin; P = 0.038; Fig. 4a). This improved outcome correlated with higher response rates to this therapy (first line CR/CRi rates 11/13, 85% for ICT + midostaurin vs. 19/38, 50% for ICT only; P = 0.048; Fig. 4b). Statistical significance got lost after censoring for allo-HSCT (median survival 126 days for ICT vs. 139 days for ICT + midostaurin; P = 0.0835; Fig. 4c); however, it has to be noted that the vast majority of FLT3-mutated patients were allografted in CR1 at our division.
Fig. 4
Addition of novel substances to ICT. Comparison of overall survival between patients treated with intensive chemotherapy (ICT) ± midostaurin (a, Mido) and ± gemutuzumab ozogamicin (d, GO). Comparison of overall survival censored for allogeneic hematopietic stem cell transplantation (allo-HSCT) between patients treated with ICT ± Mido (b) and ± GO (e). Cumulative CR/CRi rates in ICT-treated patients ± Mido (c) and ± GO (f)
Another targeted treatment approach licensed between 2013–2023 is gemtuzumab ozogamicin (GO). It is again added to ICT regimens and has been licensed for CD33-positive AML by the EMA in 2018 [27, 28]. The ALFA-0701 licensing trial showed the most prominent benefit of GO addition within the favorable and intermediate-risk groups [27]. Consequently, international guidelines like Onkopedia recommend its use only within these AML subgroups (https://www.onkopedia.com/). As this strategy is followed at our division, we focused on comparing intensively treated patients with and without GO in these risk groups (n = 15 patients ICT + GO vs. 51 patients ICT only). Addition of GO resulted in a trend to longer OS, although statistical significance was not reached (median survival 1025 days for ICT vs. median survival not reached for ICT + GO; P = 0.088; Fig. 4d). In agreement with the ALFA-0701 licensing trial [27], we failed to observe differences in CR/CRi rates between ICT and ICT + GO (first line CR/CRi rates 13/15, 87% for ICT + GO vs. 33/51, 65% for ICT only; P = 0.124, Fig. 4e); however, after censoring for allo-HSCT, the addition of GO to ICT correlated with a significant elongation of survival, suggesting that particularly patients without allografting profit from this combination (median survival 381 days for ICT vs. median survival not reached for ICT + GO; P = 0.049; Fig. 4f).
Other agents licensed between 2013–2023 were either not molecularly targeted (such as CPX-351 [29]), not available until the data cut-off in April 2023 (quizartinib) or not used as first line approaches in patients eligible for ICT and were therefore not analyzed in this study.
For nonintensively treated patients, the hypomethylating agents azacitidine (AZA) and decitabine (DEC) were used throughout the 2013–2023 observation period [30,31,32]. Like all other treatments employed (ICT and venetoclax/HMA), HMA monotherapy also proved to be efficacious and prolonged the OS compared with best supportive care (Supplementary Fig. 4). In this respect, we did not observe a difference in CR/CRi rates or OS between the HMAs AZA and DEC (CR rates: 3/32, 9% for AZA vs. 2/16, 13% for DEC, P = 0.738; OS: median survival 198 days for AZA vs. 146 days for DEC, P = 0.872; Supplementary Fig. 5). Venetoclax (VEN) was added to eligible patients (see VIALE‑A licensing trial for details [14]) after its licensing by the EMA in 2021. We could compare the outcomes of 48 patients treated with HMA monotherapy and 21 patients treated with HMA/VEN. The CR/CRi rates were significantly improved in the HMA/VEN group (5/48, 10% for HMA vs. 11/21, 52% for HMA/VEN, P < 0.001; Fig. 5a). This improved treatment response did not correlate with a better OS in patients treated with HMA/VEN (median survival 198 days for HMA vs. 171 days for HMA/VEN, P = 0.167; Fig. 5b); however, this analysis might have been biased by the small cohort size and the short observational period in the HMA/VEN group. Due to missing EMA licensing, LDAC/VEN [33] was not used in our hospital. Moreover, other novel licensed and targeted treatment approaches (including ivosidenib for IDH1-mutated patients [13]) were not available during the observation period 2013–2023 (data cut-off 19 April 2023).
Fig. 5
Outcome data of combining hypomethylating agents (HMA) with venetoclax (VEN). a Cumulative CR/CRi rates and b overall survival (OS) of patients treated with HMA monotherapy and HMA/VEN combination. c Cumulative CR/CRi rates in patients treated with ICT and VEN/HMA. d Comparison of OS between patients treated with intensive chemotherapy (ICT) and VEN/HMA. e Comparison of OS censored for allogeneic hematopoietic stem cell transplantation (allo-HSCT) between patients treated with ICT and VEN/HMA
While HMA/VEN nowadays has been established as the gold standard for ICT-ineligible AML patients, recent data might also warrant its use in specific subgroups of patients eligible for ICT and allo-HSCT. Based on these data, the current National Comprehensive Cancer Network (NCCN) guidelines (version 4.2023, https://www.nccn.org/guidelines/category_1) enable its use in patients with poor risk constellation. This regimen has also been followed in our institution for older patients ≥ 60 years and adverse ELN2022 risk stratification and enabled the comparison of ICT and HMA/VEN within this high-risk cohort (n = 10 for HMA/VEN vs. n = 32 for ICT). Interestingly, CR/CRi rates were similar between the groups (12/32, 38% for ICT vs. 4/10, 40% for HMA/VEN, P = 0.887, Fig. 5c). Regarding OS, there was a trend for longer survival in patients treated with ICT; h, statistical significance was not reached (median survival 407 days for ICT vs. 136 days for HMA/VEN, P = 0.071, Fig. 5d). This trend to extended survival in patients treated with ICT was lost when OS was censored for allo-HSCT (median survival 275 days for ICT vs. 136 days for HMA/VEN, P = 0.418, Fig. 5e), suggesting that the improved survival of older adverse-risk patients treated with ICT might be mediated by consolidation with allo-HSCT.
留言 (0)