
記住我




The NHANES is a nationally representative survey that assesses the health and nutritional status of non-institutionalized civilians in the U.S. It includes demographic data, dietary data, physical examinations, and health-related information. It combines interviews initially conducted at the participant’s home, followed by health examinations conducted at the Mobile Examination Center. The sampling methods, weights, and details of data collection can be found on its official website [15]. To ensure the representativeness and validity of our research findings, we considered the sampling and weighting procedures in our study. All analyses used weighted samples (“wtdr2d”). Furthermore, stratification and primary sampling units (PSUs) were incorporated into our analysis to account for the complex survey design of the NHANES. Stratification ensures that subgroups within the population are adequately represented, whereas PSUs help maintain the integrity of the sampling frame and reduce sampling error. By combining these factors, we were able to generate estimates that are more accurately representative of the U.S. population. The present study was based on the analysis of NHANES data from 2009 to 2018. The NHANES research plan was approved by the Ethics Review Committee of the National Center for Health Statistics (NCHS). Prior to the interview and inspection steps, each participant signed an informed consent form.
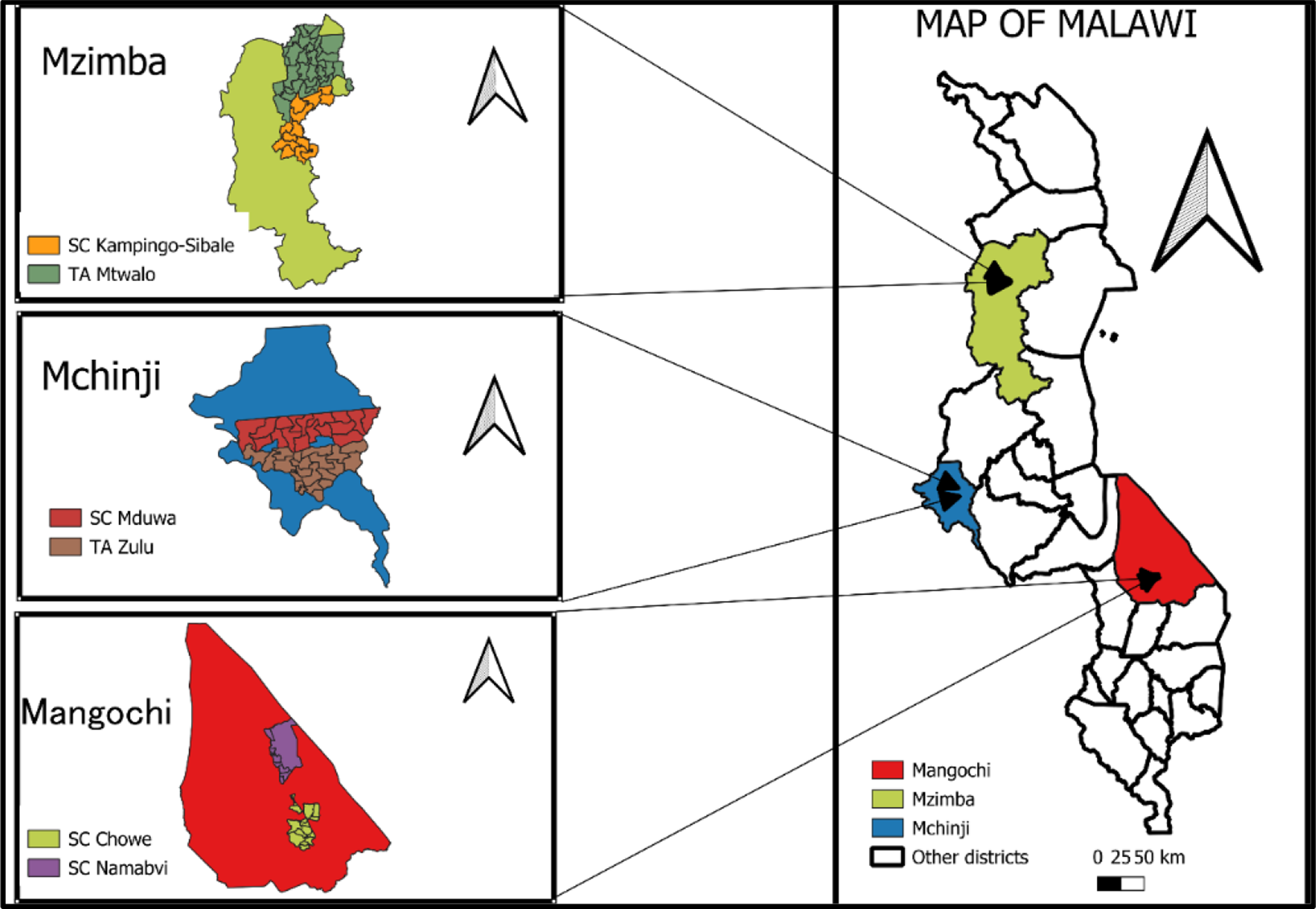
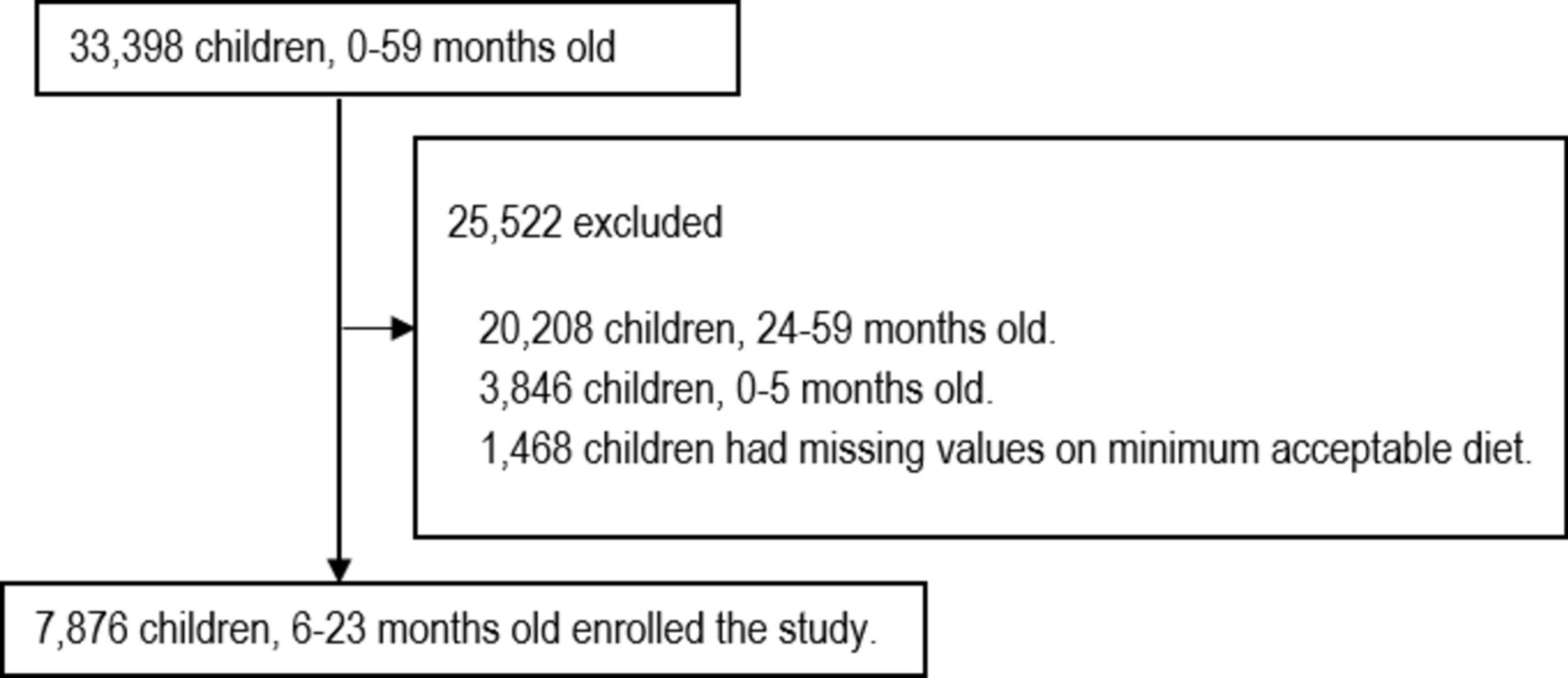
Among the 49,693 participants in the NHANES database from 2009 to 2018, 28,835 were adults (age ≥ 20), and 22,119 had complete dietary iron data and HF questionnaire data. Among these 22,119 subjects, 727 were excluded because their iron intake exceeded the tolerable upper intake level of > 45 mg/day [16, 17]. In addition, we excluded pregnant and breastfeeding populations because pregnancy and breastfeeding might alter indicators such as dietary intake and body weight. An extremely small number of missing covariates, such as educational level and smoking were also excluded. Our study ultimately included 20,853 American adult participants. (Fig. 1)
Fig. 1
Flow chart of participant selection. Abbreviations: NHANES, National Health and Nutrition Examination Survey
Assessment of dietary iron intakeDietary iron intake was assessed via two 24-h dietary recall interviews. The Mobile Examination Center was the site of the initial dietary interview, and the second interview was conducted telephonically after 3–10 days. Each participant’s total daily energy and nutrient intake from food and beverages were calculated, along with data indicating whether their food intake was normal. These details were compiled into the total nutrient intake file for analysis. The 24-h dietary supplement use section was used to obtain information from NHANES participants on the type and amount of dietary supplements consumed 24 h before the interview and to estimate the amount of nutrients consumed from these dietary supplements to estimate nutrient intake. In accordance with the NHANES protocol, the mean total nutrient intake from two 24-h dietary recall interviews and the mean total dietary supplements from two 24-h dietary supplement uses were combined to assess nutrient intake as accurately as possible. Only participants who provided complete data for both 24-hour dietary recall interviews and two 24-hour dietary supplement uses were included in the study. For these participants, the average of the two assessments of total dietary iron intake was calculated and used in the analysis. In this study, dietary iron intake was further divided into quartiles.
Assessment of HFIn accordance with previous NHANES-based studies, participants who were asked in the health questionnaire “Has a doctor or other health professional ever told you that you had congestive HF?,” and those who answered “yes” were considered to have HF [18].
CovariatesWe screened nine possible confounding factors related to HF and dietary iron: age, gender, race/ethnicity, educational level, smoking, alcohol consumption, body mass index (BMI), hypertension, and diabetes mellitus (DM). Ethnicity was divided into five categories: non-Hispanic white, non-Hispanic black, Mexican American, other Hispanics, and others. Educational level was divided into three categories: college or above, high school or equivalent, and less than high school. The degree of smoking was classified according to the following indicators: [1] never: smoked fewer than 100 cigarettes in life; [2] former: smoked more than 100 cigarettes in life but did not smoke at all; [3] now: has smoked more than 100 cigarettes in life and smokes some days or every day. The daily alcohol consumption data are the average of the alcohol consumption data from the two 24-hour dietary recall interviews. BMI was calculated by dividing weight in kilograms by the square of height in meters and then rounding it to one decimal place. Hypertension was defined when an individual met at least one of the following three criteria: [1] used antihypertensive drugs [2], was diagnosed with high blood pressure by a doctor, and [3] had a mean blood pressure higher than 130/80 mmHg. The average blood pressure was obtained as described in the NHANES. It was calculated via the following protocol: the diastolic reading with zero was not used to calculate the diastolic average. If all diastolic readings were zero, the average was zero. If only one blood pressure reading was obtained, it was considered the average. In the case of more than one blood pressure reading, the first reading was always excluded from the average. There were four types of diabetes: none, impaired glucose tolerance, impaired fasting glucose, and DM. DM was defined in this article as meeting at least one of the following criteria: having been diagnosed with diabetes by the doctor, glycosylated hemoglobin type A1C (HbA1c) (%) ≥6.5, fasting glucose (mmol/L) ≥7.0, random blood glucose (mmol/L) ≥11.1, 2-h oral glucose tolerance test blood glucose (mmol/L) ≥11.1, or the use of diabetes-related medication or insulin. BMI was measured by experts using routine physical examination techniques.
Statistical analysesWe used the R programming language (version 4.3.2) for all the statistical analyses. The statistical significance was determined as two-tailed, with P < 0.05. The analysis method was similar to that used in a previous study [19] as follows: Participants were divided into four groups according to the quartile of iron intake (Q1–Q4). The continuous variables associated with the covariates are expressed as the means (standard errors), and the categorical variables are expressed as quantities (percentages). The baseline differences between the continuous and categorical variables were assessed using ANOVA and χ2 tests, respectively. We adjusted the weights in the analysis to prevent oversampling and reduce non-response. Univariate and multivariate logistic regression models were used to analyze the relationships between HF and iron intake in all participants and different subgroups, taking covariates into account, and were divided into three models: the model with unadjusted covariates; Model 1 adjusted for gender, age, race and education level; and Model 2 was fully adjusted for covariates. To assess the dose‒response relationship between dietary iron intake and heart failure, restricted cubic spline (RCS) was used. In addition, a stratified analysis was performed, taking into account age, gender, ethnicity, smoking, alcohol consumption, hypertension and DM.
留言 (0)