
記住我







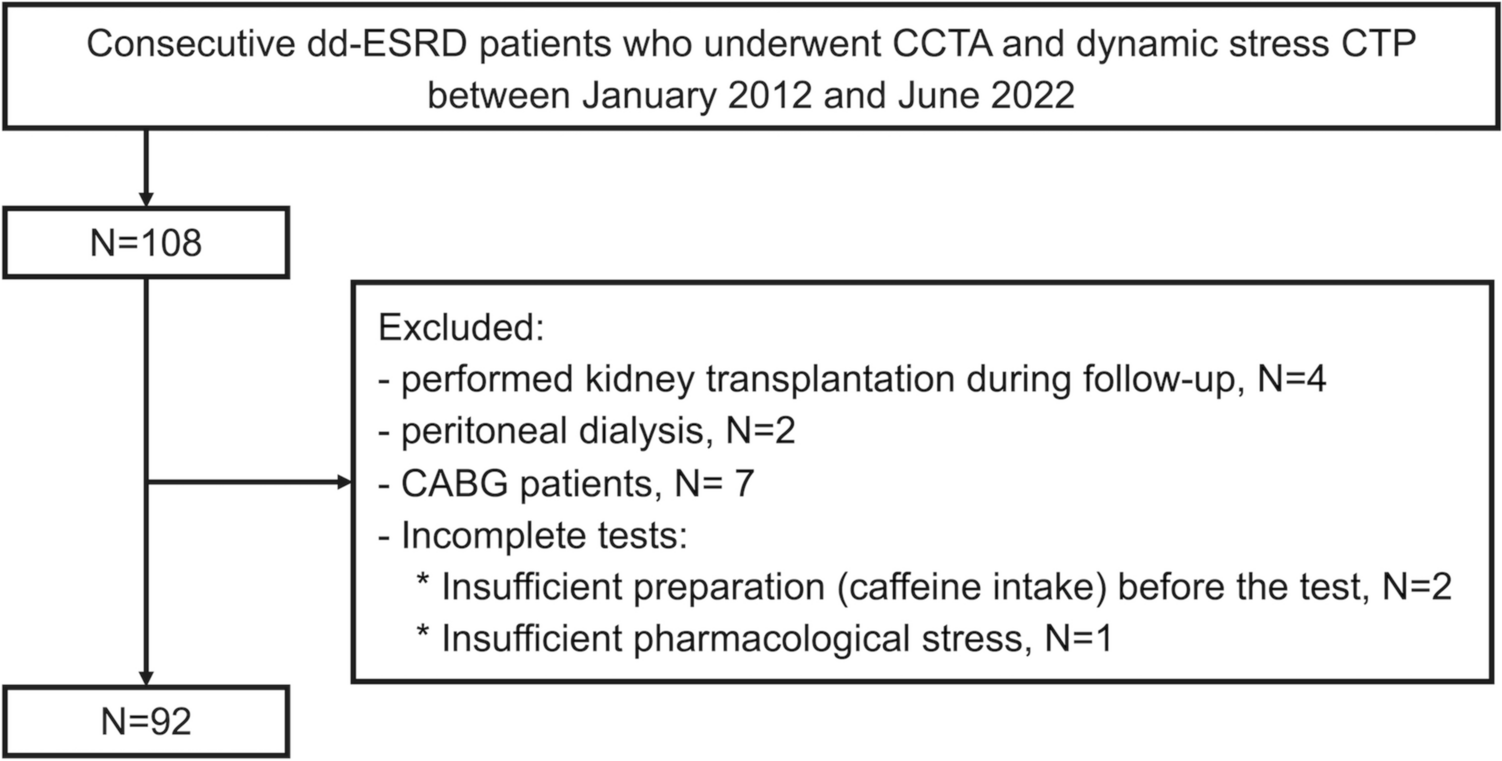
Our institutional review board approved this retrospective study, and the institutional ethics committee waived the requirement for informed consent. A total of 61 consecutive patients who underwent liver MRI with Gd-EOB-DTPA between May and September in 2023 were identified. Among these, 54 patients with focal hepatic lesions were included in this study. The patient population consisted of 36 men and 18 women (mean age, 70.5 years; range, 18–93 years) (Fig. 1). The reasons for liver MRI were surveillance or follow-up for hepatocellular carcinoma in cirrhosis (n = 24), focal hepatic lesions detected on CT (n = 9), and evaluation of metastasis (n = 21). Demographics of study population are shown in Table 1.
Fig. 1
Flowchart of patient selection
Table 1 Demographics of study populationMRI techniqueMRI was performed in all patients using a 3-T MR system (Vantage Centurian; Canon Medical Systems, Otawara, Japan). BH dynamic contrast-enhanced (CE) 3D T1-weighted GRE imaging with FS was conducted before and after the intravenous administration of Gd-EOB-DTPA (0.1 mg/kg, EOB Primovist; Bayer Phama, Osaka, Japan). The contrast material was injected using a power injector at rate of 1.0 mL/s, and flushed with 20 mL of saline. Multiphasic images were obtained during the arterial, portal venous, transitional, and hepatobiliary phases after intravenous injection. HBP images with FS using CS and AiCE were acquired 20 min after bolus injection, and then high-precision HBP imaging with FS using the modified Fast 3D mode wheel and PIQE was performed immediately after HBP imaging using CS and AiCE. The MRI parameters for HBP imaging using CS and AiCE and high-precision HBP imaging using the modified Fast 3D mode wheel and PIQE are shown in detail in Table 2. In addition, BH multi-shot T2-weighted fast spin-echo (FSE) images with FS (repetition time [TR]/echo time [TE]: 4000/90; flip angle: 90°; slice thickness: 5 mm; field of view [FOV]: 300 × 360), BH single-shot T2-weighted FSE images with FS (TR/TE, 17,000/60; flip angle, 90°; slice thickness, 5 mm; FOV, 300 × 360), and respiratory-triggered diffusion-weighted images (DWI) (TR/TE: 2300/42; slice thickness: 6 mm; FOV: 280 × 380) were obtained between the transitional phase and the hepatobiliary phase as part of the routine liver MRI protocol.
Table 2 MR parameters for standard HBP images using CS and AiCE and high-precision HBP imaging using modified Fast 3D mode wheel and PIQEQualitative analysisThree radiologists with 8, 21, and 35 years of experience in abdominal MRI, respectively, reviewed images from both the standard HBP using CS and AiCE and the high-precision HBP using the modified Fast 3D mode wheel and PIQE. The radiologists were blinded to the MR parameters, laboratory data, patient histories, and final diagnoses. Three reviewers independently scored the following parameters using a 5-point rating scale: image noise (1 = nondiagnostic due to severe noise, 2 = moderate noise causing substantial impact on the diagnosis, 3 = mild noise causing little impact on the diagnosis, 4 = minimal noise, 5 = no noise), the presence of artifacts and motion-related blurring (1 = nondiagnostic due to severe artifacts, 2 = moderate artifacts causing substantial impact on the diagnosis, 3 = mild artifacts causing little impact on the diagnosis, 4 = minimal artifacts, 5 = no artifacts), conspicuity of liver contours and intrahepatic structures (1 = mostly invisible, 2 = partly invisible, 3 = unclearly visible, 4 = almost clearly visible, 5 = clearly visible), and overall image quality (1 = non-diagnostic, 2 = poor, 3 = acceptable, 4 = good, 5 = excellent). Regarding hepatic lesion identification, 2 investigators with 4 and 11 years of experience in abdominal MRI, respectively, recorded all visible focal hepatic lesions (≥ 5 mm, maximum 10 lesions per patient). Pathological examinations were not performed to confirm lesions identified as focal hepatic lesions. The determination of the presence of true lesions was made by 1 radiologist (study coordinator: 21 years of experience in abdominal MRI) after reviewing clinical-laboratory information, other MR sequences, and follow-up examinations.
Quantitative analysisQuantitative measurements were performed by one radiologist (M.T.) on a workstation (Shade Quest; FUJIFILM Medical Solutions, Tokyo, Japan). A circular or oval region of interest (ROI) (50–200 mm2 according to the target lesion or organ) was placed in the liver parenchyma, as well as a hepatic lesion (the largest lesions if multiple lesions were observed) at the same slice level where the hepatic lesion was present. Large vessels, bile ducts, and any artifacts were avoided to compare the noise (standard deviation: SD) of the liver, signal-to-noise ratio (SNR) of the liver, and contrast-to-noise ratio (CNR) between standard HBP imaging using CS and AiCE and high-precision HBP imaging using the modified Fast 3D mode wheel and PIQE. The SNR of the liver and CNR were calculated using the following formulas:
$$} = }\left( }} \right)}} \mathord}\left( }} \right)}} }}} \right. \kern-0pt} }}.$$
$$} = }}} \right)} \mathord}}} \right)} }}} \right. \kern-0pt} }}.$$
Statistical analysesQuantitative and qualitative factors were compared using the Wilcoxon signed-rank test. p values of < 0.05 were considered to indicate statistical significance. Inter-reader reliability was calculated using the Fleiss kappa test. The Fleiss kappa value was interpreted as follows: 0.81–1.00, excellent agreement; 0.61–0.80, substantial agreement; 0.41–0.60, moderate agreement; 0.21–0.40, fair agreement; < 0.20, poor agreement. All data were analyzed using SPSS (version 27.0; IBM, Armonk, NY, USA).
留言 (0)