
記住我







Quantitative susceptibility mapping (QSM) is a post-processing technique to quantitatively estimate local magnetic susceptibility in biologic tissue using gradient-recalled echo (GRE)-phase measurement [1,2,3,4]. QSM provides quantitative information on magnetic susceptibility which is useful for differentiating between paramagnetic and diamagnetic susceptibility. QSM has proven to be a valuable tool for assessing the deposition of paramagnetic substances, such as iron deposition, hemosiderin, gadolinium, and diamagnetic substances, such as calcification and myelin [5,6,7,8]. QSM has thus been applied for evaluating various conditions, such as microbleeds [9, 10], iron accumulation associated with aging changes [11,12,13], gadolinium deposition [14, 15], and neurodegeneration such as Parkinson’s disease [16, 17]. Although the usefulness of QSM is well established, QSM has not yet seen common use in clinical practice, partly because of the long scan time [18].
Parallel imaging techniques such as generalized autocalibrating partially parallel acquisition (GRAPPA) and sensitivity encoding (SENSE) have been introduced to reduce scan time and preserve signal-to-noise ratio (SNR) [19, 20]. By taking advantage of coil sensitivity encoding from multi-channel receiver coils, GRE with an acceleration factor of 2 is generally applied for QSM with parallel imaging techniques such as SENSE and GRAPPA, but the ability to reduce scan time for QSM with GRE remains limited. Using other sequences such as 3D echo planar imaging (EPI), scan times for QSM data can be reduced to around 2 min [9]. In a multi-shot approach with short EPI train lengths, distortion and blurring become limited, and images with a considerable gain in both SNR and coverage as compared to GRE imaging can be obtained within a given amount of scan time [21]. The disadvantage of 3D EPI is the data acquisition at only one echo time. On the other hand, higher acceleration for QSM with GRE has not been evaluated in detail. Recently, wave-controlled aliasing in parallel imaging (CAIPI) acquisition enables highly accelerated volumetric imaging with fewer artifacts and low SNR penalties by playing sinusoidal gradients during the readout of each phase encoding line [22,23,24,25,26,27,28,29]. The acceleration factor for wave-CAIPI has been reported as ninefold at most (threefold for phase encoding, threefold for slice encoding).
More acceleration for GRE has been expected to create QSM using wave-CAIPI, and several reports have described susceptibility-weighted imaging (SWI) with wave-CAIPI [30, 31]. Using wave-CAIPI, higher spatial resolution than the previous 3D EPI report can be achieved at 3 T with a scan time less than 2 min [21, 31]. However, QSM with wave-CAIPI has not been evaluated in detail in clinical practice [32]. We hypothesized that QSM with ninefold acceleration using wave-CAIPI could be used reliably in clinical scanners in terms of reproducibility and consistency. The purpose of this study was to compare QSM with wave-CAIPI 9 × (QSM_WC9 ×) with the reference standard QSM with GRAPPA 2 × (QSM_G2 ×) in two MR scanners. We also compared the detectability of microbleeds in both QSMs to demonstrate clinical feasibility of both QSMs.
Materials and methodsThis prospective study was performed in accordance with the Declaration of Helsinki and was approved by Kyoto University Graduate School and Faculty of Medicine, Ethics Committee. Written informed consent was obtained from each subject.
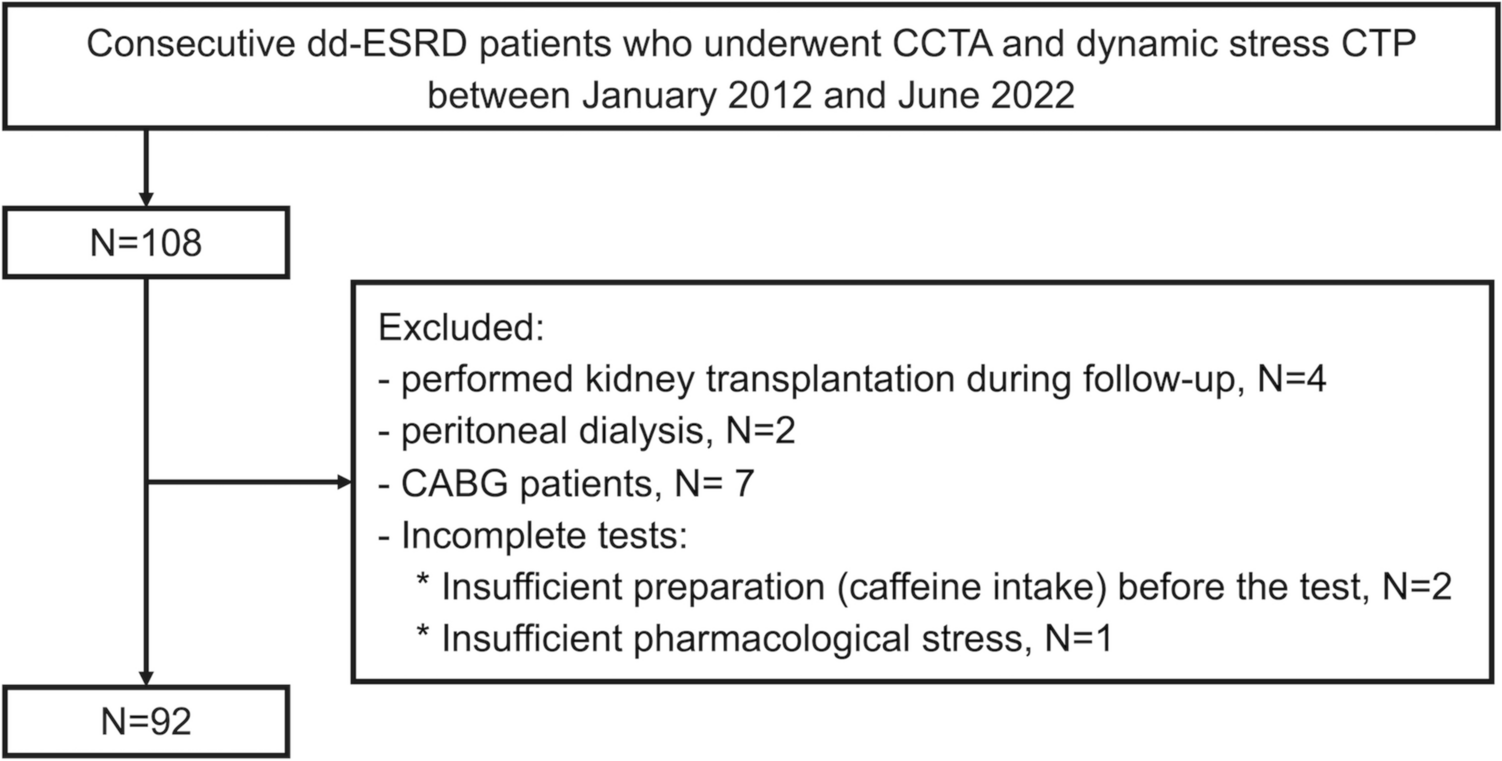
Healthy subjectsHealthy subjects were recruited to evaluate: (1) intra-scanner reproducibility; (2) inter-scanner consistency; and (3) inter-sequence consistency of QSM_G2 × and QSM_WC9 × . Exclusion criteria for these healthy subjects were as follows: (1) severe head motion during imaging; or (2) incidental findings such as cerebral infarction, old hemorrhage, and other abnormalities. In total, 55 healthy subjects (34 men, 21 women; mean age, 38.3 years; range, 23–79 years) were included in this study (Fig. 1).
Fig. 1
Enrollment of healthy subjects and patients
Analysis 1, intra-scanner reproducibility (single scanner, test and re-test) (n = 8)Intra-scanner reproducibility was analyzed with the test and re-test data of a subject who underwent two scans with a single MR unit (Scanner A). QSM_G2 × (1st scan, 2nd scan), and QSM_WC9 × (1st scan, 2nd scan) were evaluated, respectively (n = 8). Note that head position differed between 1st scan and 2nd scan.
Analysis 2, inter-scanner consistency (different scanners, same sequence) (n = 19)Inter-scanner consistency was analyzed using data from subjects who underwent scans with 2 MR units (Scanners A and B) (n = 19). QSM_G2 × (Scanner A and B) and QSM_WC9 × (Scanner A and B) were both evaluated. Note that head positions differed, since the data were obtained from different scanners.
Analysis 3, inter-sequence consistency (same scanner, different sequences) (n = 28)Subjects (n = 28) underwent MR scans with both Scanner A (n = 14) and Scanner B (n = 14). QSM_G2 × and QSM_WC9 × were evaluated with Scanner A. QSM_G2 × and QSM_WC9 × were also evaluated with Scanner B. Note that head position did not change during the two sequences.
These subjects also underwent GRE with GRAPPA 9 × and GRE with CAIPI 9 × , then QSM_G9 × and QSM_C9 × were created, respectively. However, these data were not included for analyses due to severe parallel imaging artifacts that were always present (representative figures with QSM_G9 × and QSM_C9 × are shown in Supplemental Fig. 1).
PatientsPatients for whom SWI was requested between July 2019 and August 2020 were also recruited in this study to measure microbleeds on QSM_G2 × and QSM_WC9 × . Exclusion criteria for these patients were as follows: 1) severe head motion; or 2) more than 30 microbleeds. Three patients with brain contusion (n = 2) and cerebral amyloid angiopathy (n = 1) were excluded due to too many microbleeds. Sixty patients (30 women, 30 men; age, 55.4 years; range, 21–85 years) were finally enrolled in this prospective study (Fig. 1).
MR imagingMR imaging was performed with two 3-T MR scanners (MAGNETOM Prisma; Siemens Healthineers, Erlangen, Germany) with a 64-channel head/neck coil in our institute (Scanners A and B). Imaging with 3D gradient echo (GRE) sequences was performed using the following parameters in common: TR, 32 ms; TE, 20 ms; flip angle, 15°; bandwidth, 80 Hz/pixel; field of view, 230 × 230 mm2; matrix, 320 × 294; spatial resolution, 0.72 × 0.72 × 1.0 mm3. For acceleration, 24 reference lines were acquired in the phase-encoding direction for all GREs, and reference lines in slice direction (and scan time) were as follows: (1) GRE with GRAPPA 2 × 1 (GRE_G2 ×), not accelerated in slice direction (6 min 8 s); (2) GRE with a prototype wave-CAIPI 3 × 3 (GRE_WC9 ×), using 24 reference lines in slice direction with a CAIPI shift factor of 1 (1 min 25 s).
Images were also obtained using 3D T1-magnetization prepared rapid acquisition gradient-echo (MPRAGE), with: TR, 2300 ms; TE, 4.67 ms; flip angle, 9°; and bandwidth, 130 Hz/pixel. Spatial resolution was isotropic voxel of 0.9 mm, and 208 slices were acquired. For acceleration, 24 reference lines were acquired in the phase-encoding direction for all MPRAGEs (GRAPPA 2 × 1), and not accelerated in slice direction. Scan time was 5 min 21 s.
Post-imaging analysis for healthy subjectsQSM was created from magnitude and phase images of 3D GRE using STI Suite version 3 (https://people.eecs.berkeley.edu/~chunlei.liu/software) (Fig. 2). Laplacian-based phase unwrapping, variable-kernel sophisticated harmonic artifact reduction for phase data, and dipole inversion were performed, and then, QSM was created [4]. The 3D-MPRAGE images were registered to 3D GRE images of the corresponding magnitude. Registered 3D-MPRAGE images were segmented to create a Diffeomorphic Anatomical Registration Through Exponentiated Lie Algebra (DARTEL) template using SPM12 (https://www.fil.ion.ucl.ac.uk/spm/software/spm12/). This template was used to normalize QSM to the MNI space and perform average QSM among patients.
Fig. 2
Post-imaging analysis for healthy subjects. QSM was created from magnitude and phase images of corresponding 3D GRE (G2 × and WC9 ×). After performing Laplacian-based phase unwrapping, variable-kernel sophisticated harmonic artifact reduction for phase data, and dipole inversion, QSM was created. Next, 3D-MPRAGE images were registered to 3D GRE images of the corresponding magnitude. Registered 3D-MPRAGE and QSM were normalized to the MNI space
The following volumes of interest (VOIs) were then applied to QSM: splenium of the corpus callosum, caudate nucleus, putamen, optic radiation, internal capsule, globus pallidus, substantia nigra, red nucleus, and dentate nucleus (Supplemental Fig. 2).
Evaluation of microbleeds in patientsPatients underwent QSM_G2 × and QSM_WC9 × in either of the two MR units. Microbleeds were evaluated by two raters (A.S. and K.P.W., each with 9 years of experience in neuroradiology). If the raters detected microbleeds, the number of microbleeds was compared. In the case of discrepancies between the two raters, the number of microbleeds was determined by another radiologist (Y.F., with 25 years of experience in neuroradiology).
Calculation of SNRCalculation of SNR was performed by serial measurements of GRE sequences for the spherical phantom (NiSO4·6H2O). Specifically, GRE_G2 × , GRE_WC9 × , GRE_C9 × , and GRE_G9 × were measured 10 times and the SNR map was created with the mean value divided by the standard deviation.
Statistical analysisIntraclass correlation coefficient (ICC) and 95% confidence intervals (CIs) of susceptibility values were calculated. Bland–Altman analysis was performed for susceptibility values. The inter-observer agreement for detection of microbleeds was assessed with ICC.
Statistical analysis was performed using MedCalc version 18 (MedCalc Software, Ostend, Belgium) and JMP Pro version 16.0 (SAS Institute Inc., Cary, NC, United States).
留言 (0)