
記住我






There are many factors that may significantly impact the results of epidemiological studies, such as population density, geographic region, economic status, and cultural differences. Similarly, sociodemographic variables may influence the etiology, incidence, clinical presentation, and treatment strategies of maxillofacial fractures [9]. Hence, the epidemiological features of maxillofacial fractures vary across—and even within—countries [10].
Istanbul, which constitutes 18.33% of Turkey's population and has around 15 million residents, is bifurcated into two regions: the Anatolian and European sides. The area around our hospital is a rather underdeveloped part of Istanbul, characterized by low socioeconomic factors, inadequate educational attainment, and a high incidence of criminal activity. Despite our hospital's proximity to a relatively underdeveloped area of Istanbul concerning sociocultural factors, it receives referral patients from districs on the Anatolian side and less frequently also from the European side. As the preeminent maxillofacial institution on the Anatolian side, the data from our hospital is anticipated to reflect the totality of Istanbul. But to assess the assaults regarding their substantial contribution to the etiology, it is essential to acquire current district-based crime statistics for Istanbul and retrospectively identify the regions where the patients reside.
Previous studies from various regions of Turkey have reported similar male-to-female ratios and mean ages in maxillofacial trauma cases as observed in our study [11,12,13,14]. However, while RTAs are typically the leading cause in other regions in Turkey and also developing countries [11, 12, 15,16,17], our study found assault was the leading known cause of maxillofacial fractures (29.1%), followed by falls (26%) and RTAs (16.5%) similar to developed countries. Although factors such as age and gender remain consistent, the difference in etiology highlights the need for multicenter studies across Turkey to gain a more comprehensive understanding of the demographic and clinical characteristics of maxillofacial trauma nationwide.
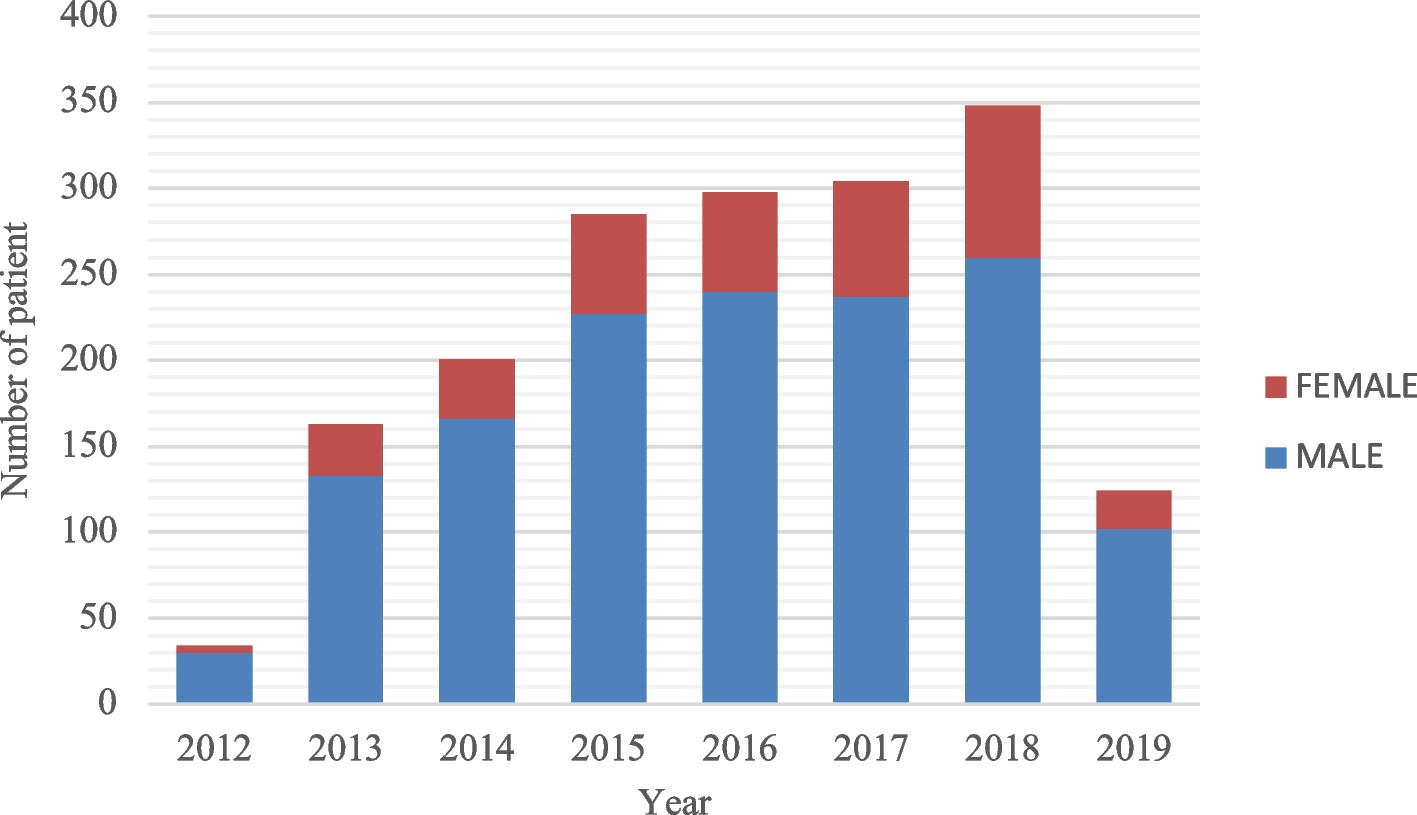
The comparison between patient distribution in our study and Turkey’s 2012 and 2019 population pyramids reveals a noticeable mismatch, as shown in Fig. 2. This discrepancy is likely due to the small sample size of 1,757 patients, which is insufficient to represent the national population accurately. Additionally, maxillofacial trauma predominantly affects young adults, which skews the age distribution compared to the general population. For more accurate results, future studies should include larger sample sizes or use national databases to better reflect both condition-specific and overall population demographics.
Fig. 2
Comparison of Age and Gender Distribution Between Maxillofacial Trauma Patients and Turkey's General Population. The left panel shows the age and gender distribution of Turkey's general population in 2012, while the middle panel represents the distribution of the maxillofacial trauma patients treated between 2012 and 2019. The right panel illustrates the age and gender distribution of Turkey's general population in 2019. Data for Turkey's general population were sourced from the Turkish Statistical Institute (TÜİK) for 2012 and 2019
Men experience maxillofacial trauma significantly more than women all over the world and in all regions [18, 19]. While the male-to-female patient ratio is relatively high in underdeveloped and developing countries, it is lower and approaches 1:1 in developed countries. However, even in developed countries, men experience maxillofacial trauma almost twice as much as women. The male-to-female patient ratio is relatively high in underdeveloped and developing countries, while in developed countries, men experience maxillofacial trauma almost twice as often as women. In the literature, the male-to-female patient ratio ranges from 2:1 to 9.6:1 [5,6,7, 17, 20]. In the present study, the ratio was 3.9:1. In our study, the overall ratio was 3.9:1, which contrasts with findings from neighboring Middle Eastern countries, where ratios between 4.5:1 and 11:1 have been reported [21,22,23]. Excluding the statistics from 2012, when the ratio peaked at 7.5:1 due to a small sample size (34 patients), the annual male-to-female ratios observed in our study fluctuated between 4.7:1 and 3:1, with no statistically significant variation over time. The gender distribution found in our study is closer to that reported in urbanized European countries [24, 25]. This suggests that the greater involvement of women in society in Turkey, compared to other Middle Eastern countries, may increase their risk of experiencing trauma. In the European Maxillofacial Trauma (EURMAT) project [7], a multicenter prospective study including data from 13 hospitals across Europe, a mean male-to-female patient ratio of 3.6:1 was documented, which is similar to the ratio found in our study. However, in the EURMAT project, the ratio varied widely across the different centers and countries, with the maximum value encountered in Kiev (9.4:1) and the minimum value in Amsterdam (2.2:1) [7].
The etiology is an important epidemiological factor of maxillofacial fractures that directly affects the treatment modality, incidence, and clinical presentation. In the present study, assault was the leading known cause of maxillofacial fractures (29.1%), followed by falls (26%) and RTAs (16.5%). Studies have shown that in developing countries, the most common etiology of maxillofacial trauma is RTAs [15,16,17], while in developed countries, assault and interpersonal violence are the primary causes [7, 26]. Our findings reflect those of the EURMAT project, with the two most common etiologies of maxillofacial fractures being assault and falls. The region where our hospital is located is a relatively underdeveloped area of Istanbul in terms of sociocultural factors, the education level is low, and it is an area where criminal incidents frequently occur. These factors may have contributed to the occurrence of interpersonal and household violence and an increase in the number of assault cases during the study period.
In the present study, falls constituted the second most common etiology of maxillofacial fractures. Falls were found to be the most common cause of trauma in the 0–7, 8–18, and ≥ 59 years groups. Young children may experience falls due to a lack of movement certainty and coordination, which can prevent them from adequately protecting themselves against impact [27, 28]. Our data showed that in the 8–18 years group, falls were followed by assaults. The high incidence of assaults observed among school-age children is significant. Schools should increase education on this topic, parents must be made aware, and safety must be ensured. In accordance with the findings of the EURMAT project, falls were the most common etiology among the elderly patients (≥ 59 years group) in our study. Various factors may contribute to falls in this age group, including sensory impairment, neuromuscular disorders, unsteady gait, dementia, acute illness, and postural hypotension. In the EURMAT project, falls were the most common etiology across all centers in patients aged > 40 years [7]. This was attributed to the increasing age of the European population. Various steps should be taken to reduce the incidence of falls among the geriatric population, such as conducting home safety inspections, changing medications known to affect balance, providing gait training, and improving treatable sensory impairments through educational programs [29].
Comprehending the epidemiology of maxillofacial fractures and associated injuries is essential for formulating effective preventative programs, enhancing patient care, and judiciously allocating resources [30]. The occurrence and severity of maxillofacial fractures in adults and children can be markedly diminished by the implementation of seat restraints [31]. Nevertheless, adherence, especially among young males—who are the most vulnerable—tends to be inadequate [32]. Effective interventions encompass reducing speed limits, enforcing seatbelt compliance, and promoting helmet usage with chin shields to safeguard the mandible, the bone most frequently fractured in RTAs [33]. Moreover, adults responsible for supervising youngsters should instruct them on the significance of safe practices, including the use of helmets [34]. Supplementary strategies to reduce maxillofacial injuries from RTAs in developing nations include the installation of traffic cameras, radar systems, airbags, enhanced road design (prioritizing one-way streets), segregation of traffic kinds, safer pathways for pedestrians and cyclists, and the introduction of speed bumps [33].
Geriatric patients face a heightened risk of future injuries following an initial event. Preventive interventions must encompass chronic diseases and functional limitations, including medication assessments, gait retraining, and environmental adjustments [35, 36]. Physical activity is the most efficacious strategy for fall prevention in elderly patients, and the ideal strategy is to combine it with other measures [37].
Substance abuse exacerbates increasing incidences of violent trauma. Programs aimed at preventing alcohol and drug misuse might diminish motor vehicle accidents and injuries associated with assault, resulting in health and economic advantages. Legislative actions, such increasing the legal drinking age and enforcing stronger drunk driving regulations, may contribute to a decrease in alcohol-related facial fractures[38].
Preventing osteoporosis is essential for overall health and may potentially influence maxillofacial injuries. Modifications in lifestyle, such as abstaining from smoking and limiting excessive use of alcohol and caffeine, in conjunction with regular exercise and adequate nutrition, can aid in the prevention of osteoporosis. Two categories of agents are available for its prevention and treatment: anti-resorptive and anabolic medicines[39].
We could not determine the etiology in 20.3% (male: 19.9%; female: 22%) of the patients, which is a high proportion of the cases. Since this was a retrospective study, we could not access all the data required to determine the etiology in all cases. This may be due to patients being unable to recall the trauma, especially if unconscious or confused by their injuries. Initially, patients could struggle to remember the precise origin of the trauma, particularly if they were unconscious or disoriented due to the extent of their injuries. In many instances, the trauma may have been multifactorial, leaving patients confused about which incident precipitated the injury. In emergency settings, medical teams may prioritize quick care over comprehensive history-taking, resulting in insufficient documenting of the trauma etiology. Therefore, patients with unidentified etiologies were included in the study when other clinical records were complete. Conducting prospective studies will allow for more detailed collection and analysis of etiologies.
When cases of facial trauma are analyzed according to their etiologies, the gender ratio of the patients can differ from that of the overall ratio [9]. In the EURMAT project, men accounted for more than 80% of the patients with assault-related maxillofacial injuries in centers where the percentage of assault-related maxillofacial injuries was 40% or higher [7]. In our study, 29% of the patients had assault-related maxillofacial fractures, and men accounted for 90% of the patients with assault-related maxillofacial injuries. Although the overall male-to-female patient ratio was 3.9:1 in this study, the ratio was 9:1 for assault-related fractures. This high ratio (9:1) may have been related to the high rate of alcohol and drug use among adolescent and young men in our study population. Since our study was retrospective in nature, we could not obtain sufficient data on alcohol and drug use or investigate the relationship between alcohol and drug use and maxillofacial trauma. However, it is known that the rate of alcohol and drug use is high, especially among young men, in the region where our hospital is located. Prospective studies are needed to determine this relationship.
The literature indicates that maxillofacial fractures most commonly occur in individuals aged 20–30 years [5, 9, 22, 40]. In accordance with the literature, our results showed that the highest number of maxillofacial injuries occurred in the 19–28 years group, accounting for 23.9% of all cases. However, in the EURMAT project, most centers reported that the highest number of cases occurred in groups of patients with mean ages between 30 and 39 years, and this result was attributed to the increasing life expectancy and aging of European people [7].
In terms of the fracture site, in our study, nasal fractures were the most frequently observed, accounting for 63.7% (n = 1,384) of all cases. In contrast, previous studies have indicated that the mandible is the most common fracture site in maxillofacial injuries, frequently followed by the zygoma [7, 9, 40, 41]. The main reason for this difference is that all the studies that found that mandibular fractures were the most common maxillofacial fractures were conducted in oral and maxillofacial surgery departments, whereas most patients with nasal fractures are treated either in otolaryngology or plastic surgery departments. Among all the facial bones, the nasal bones are the most vulnerable to trauma due to their location. Therefore, it is not surprising that nasal fractures are among the most frequently reported fractures in cases of maxillofacial trauma and in studies of such trauma conducted in otorhinolaryngology, plastic surgery, and EDs [42]. Given that almost all patients with maxillofacial trauma first report to an ED, it is clear that studies conducted using data collected in EDs should be the most reliable in term of analyses of fracture locations. Arslan et al. conducted their study in an ED and found that the maxillary and nasal bones were the two most commonly fractured bones in patients with maxillofacial injury [42]. Regarding our results (i.e., nasal fractures were most common, followed by maxillary fractures), we are confident that they reflect the actual types of bones fractured in patients with maxillofacial injuries in the region where our hospital is located for two reasons. First, there is no oral and maxillofacial surgery department in our hospital or near our region. Second, regardless of whether surgical intervention is required or not, almost all patients with facial fractures are referred by the ED to our department. In the EURMAT project, which only included oral and maxillofacial departments, the most commonly fractured bone was found to be the mandible; however, the EURMAT collaborators also stated that because nasal fractures are often treated by otorhinolaryngology departments, the actual epidemiological features and percentages of facial fractures may be different [7].
When we examined the reported mandibular fractures, we found that condylar-subcondylar process fractures were the most commonly observed, accounting for 36.8%. These fractures were followed by symphysis/parasymphysis, corpus, coronoid, angle, and ramus fractures in decreasing numbers. Our findings were consistent with those of the EURMAT project, where the condyle was found to be the most fractured site of the mandible (34%) [7]. Previous studies showed that the most fractured part of the mandible was the corpus [40], symphysis/parasymphysis [43, 44], or angle [45]. Notably, even though mandibular fractures ranked fifth among the types of facial fractures in our study, they were the most common fracture type that required surgical intervention with GA.
The most common treatment method used across all cases was intervention with LA (n = 825, 47%). Specifically for nasal fractures, intervention with LA was also the most frequent treatment approach (n = 813, 58.3%). For mandibular fractures, surgical intervention under GA was the most commonly employed treatment (n = 64, 54.7%). Orbital fractures were primarily managed with conservative treatment and monitoring (n = 124, 63.3%). Similarly, maxillary fractures and frontal sinus anterior wall fractures were most frequently treated with conservative management (n = 149 [65.6%] and n = 32 [54.2%], respectively).
Surgical intervention was performed in 125 patients, with the most common procedure reduction under GA (n = 40, 28.8%). It was observed that the use of surgical treatment varied significantly according to age group, particularly for the intermaxillary fixation variable in the 0–7 years group. In this group, only one patient received a plate for mandibular fractures due to concerns about hindering bone development; the plate was removed early to prevent any potential negative effects on growth. Surgical interventions were most frequently performed on the first day (n = 42). The longest period before surgery was 20 days (n = 1). Postoperative complications developed in 10 patients. The most common complications were plate exposure (n = 6, 60%), wound-site infection (n = 3, 30%), and TMJ ankylosis (n = 1, 10%). These findings highlight the importance of considering the timing and type of surgical intervention, especially in younger patients, to avoid long-term developmental issues.
The present study has some limitations. The data, which were retrospectively collected from hospital records, did not include information about the patients’ alcohol or drug use. In addition, data on the etiology of the trauma were missing for some patients; thus, the etiology was not known in 20% of cases. Therefore, further prospective studies are needed to more precisely document the proportional differences between etiologies.
留言 (0)