
記住我






This study constitutes a systematic review and meta-analysis. We formulated the research protocol following the guidelines provided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P). This meta-analysis has been registered with PROSPERO, registration number [CRD42024585756].
PICOSThe search methodology followed the PICO framework, representing P (Patient Population), I (Intervention or Exposure for observational studies), C (Comparison), and O (Outcomes). In this systematic review, we applied the PICOS approach, covering the study population (in patients undergoing orthognathic surgery), interventions (Three-dimensional virtual surgical planning of orthognathic surgery), comparison (two-dimensional conventional surgical planning of orthognathic surgery), and outcomes of interest (the accuracy of operation, surgical time) (Table 1).
Table 1 The search methodology followed the PICO frameworkEligibility criteriaComparative studies (prospective or retrospective studies and randomized controlled trials) in humans assessing the accuracy of orthognathic surgical planning using VSP compared with conventional surgical planning (CSP) were included. The inclusion criteria for this study encompassed full-text articles involving patients who underwent orthognathic surgery, specifically those that utilized three-dimensional VSP. The primary outcomes assessed were the accuracy of the operation and surgical time. Eligible study designs included clinical trials, controlled trials, retrospective and prospective studies, and case series.
To ensure the reliability and relevance of the findings, several exclusion criteria were applied. Studies were excluded if they lacked essential data on accuracy in orthognathic surgery, as incomplete data could compromise the comprehensiveness of the analysis. Articles published in languages other than English were not considered, and non-peer-reviewed literature—such as conference abstracts, posters, and unpublished studies—was excluded to maintain the quality and rigor of the evidence.
Research involving non-human subjects, including animal models, surgical simulations, and rapid prototype models, was excluded because their outcomes might not directly translate to human patients undergoing orthognathic surgery. Studies focusing on populations not representative of typical orthognathic surgery patients—such as individuals with congenital craniofacial anomalies or trauma-related injuries—were also excluded. Additionally, studies concentrating solely on procedures like genioplasty or malarplasty were not included. Studies exclusively involving pediatric patients were excluded due to differing anatomical considerations, surgical techniques, and complication profiles compared to adult patients. Research focusing solely on patients with specific medical comorbidities, such as severe cardiovascular disease or uncontrolled diabetes, was omitted to maintain a homogeneous study population and reduce confounding factors that could affect complication rates.
To include the most current evidence, studies published before a specified date were not considered. Duplicate studies or redundant data from the same study cohort were excluded to avoid repetition and to ensure the integrity of the analysis. Lastly, articles lacking complete demographic information were not included, as such information is crucial for contextualizing the study results.
Information sourcesFollowing the guidelines outlined in the PRISMA statement, we conducted an electronic search of various databases, including PubMed and Scopus. The manual search also encompassed the bibliographies of all articles chosen for full-text screening, along with previously published reviews pertinent to this systematic review. We included studies published between 2014 and 2024 in our meta-analysis. Two reviewers (LYJ and KSG) performed the study selection independently. In the event of disagreement between the reviewers, the third reviewer (OJH) was consulted.
Search strategy and article selectionA MEDLINE(PubMed) and Scopus search was conducted. The search only included articles published in English, from year 2014 until 2024. We used the Boolean operators ‘OR’ to broaden the search and ‘AND’ to combine different areas. The search equations for each database were as follows:
PubMed: ((((Accuracy) OR (precision)) AND (Orthognathic surgery)) AND (time)) OR (((Accuracy) OR (precision)) AND (orthognathic surgery)) OR ((time) AND (orthognathic surgery)).
Scopus: (TITLE-ABS-KEY(“Orthognathic surgery” AND “time”) OR TITLE-ABS-KEY((“Orthognathic surgery” AND (“Accuracy” OR “Precision”)) OR TITLE-ABS-KEY(“Orthognathic surgery” AND (“Accuracy OR Precision”) AND “time”)) AND PUBYEAR > 2013 AND PUBYEAR < 2025 AND ( LIMIT-TO (LANGUAGE, “English”)) AND (LIMIT-TO (SUBJAREA, “MEDI”) OR LIMIT-TO (SUBJAREA, “DENT”)) AND (LIMIT-TO (DOCTYPE, “ar”) OR LIMIT-TO (DOCTYPE, “cp”)).
Two independent reviewers, LYJ and KSG, evaluated the titles and abstracts of all studies found in the initial search. If the abstracts did not provide sufficient information, the reviewers examined the full text to determine whether to include or exclude the studies. The authors reviewed the full texts of all remaining articles. Any discrepancies in the results between the reviewers were resolved by consensus, and if agreement could not be reached, a third researcher (OJH) was consulted.
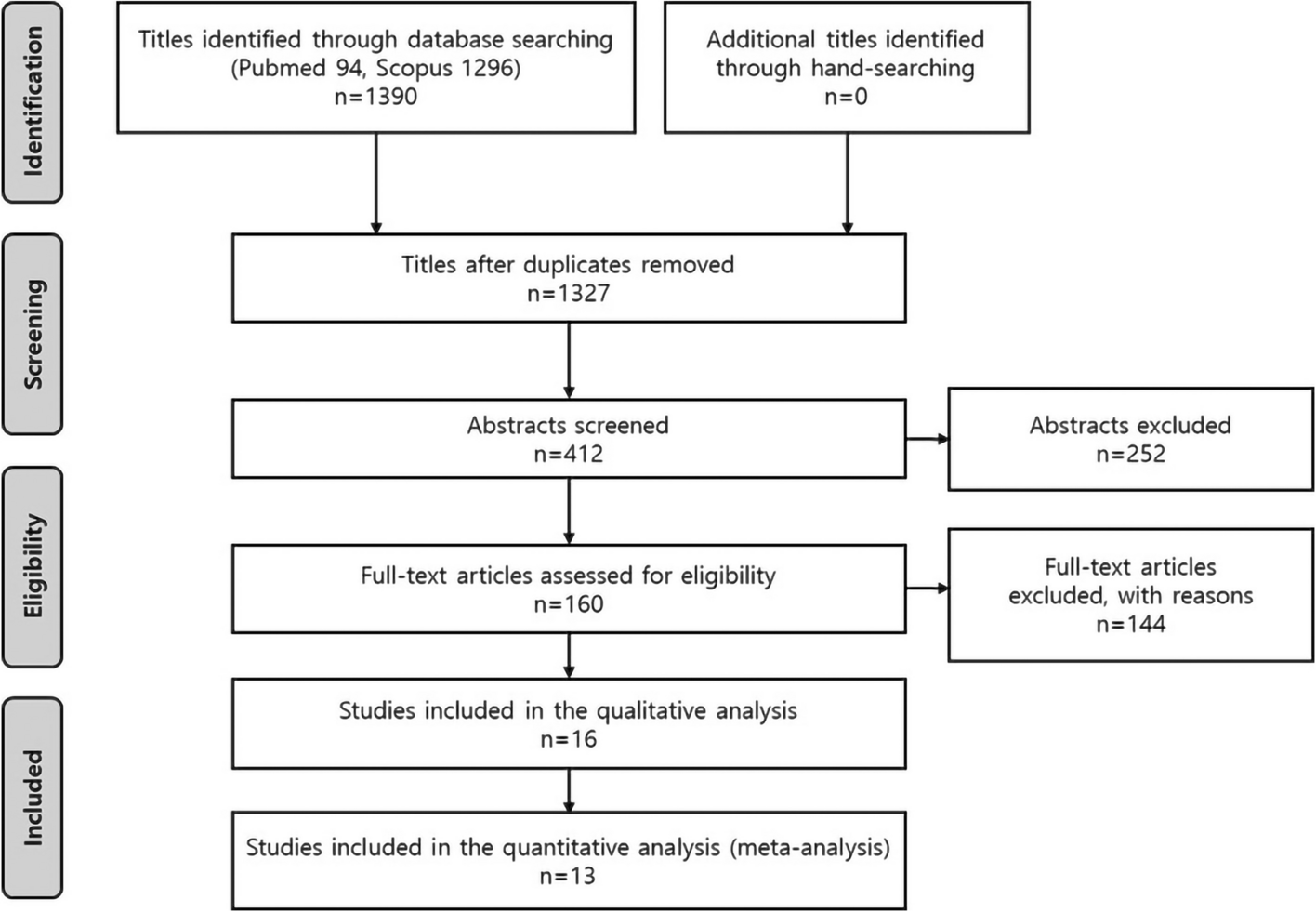
The PRISMA flow diagram provides an overview of the study selection process (Fig. 1). Initially, the titles of the identified reports were screened, and duplicates were removed. Abstracts were reviewed if the titles suggested the study was relevant. For studies that appeared relevant or if the abstract was unavailable, a full-text analysis was conducted. Additionally, the references of identified papers and previously published systematic reviews on VSP and TSP in conjunction with orthognathic surgery were cross-checked to ensure no articles were missed.
Fig. 1 Data collection process
Data collection processData were extracted by a single reviewer (LYJ) and entered into an Excel spreadsheet (Microsoft, Redmond, WA, USA). The following items were collected: first author, year of publication, journal name, study design, number of patients, mean patient age, types of experimental and control groups, imaging method, type of surgery, type of software used, and outcomes related to surgical accuracy and surgical time. The accuracy was compared using the linear absolute difference between the preoperative plan and the postoperative outcome. Surgical time was included in the meta-analysis only when it reflected the total duration of the surgery. To assess the level of agreement between the evaluators, the kappa statistic was employed using the same criteria as during the study selection phase. Any discrepancies were resolved through discussion between the evaluators; if consensus could not be reached, a third assessor (OJH) was consulted for input.
Evaluation of the study risk of biasDue to the diverse study designs of the studies included in this review, two tools were used to assess the risk of bias. The Cochrane Library Risk of Bias (RoB) tool was used for RCTs. RoBANS (Risk of Bias Assessment Tool for Non-randomized Study) tool was used for non-RCTs. There are five types of bias: selection bias, performance bias, detection bias, attrition bias, and reporting bias. The evaluation criteria for the type of bias are somewhat different between RCTs and non-RCTs (Table 2). The risk of bias was classified as either high, low, or uncertain. A risk of bias assessment was undertaken by two review authors (LYJ and KSG).
Table 2 The evaluation criteria for the type of biasStatistical analysisThe absolute mean linear difference values comparing the planned position and the postoperative position were extracted. While angular discrepancy values were included in the qualitative analysis, they were not incorporated into the meta-analysis (quantitative analysis). For absolute mean linear difference values reported as total in 3D, the data were used as is. However, when x,y values or x,y,z values, along with multiple reference points, were provided, the following formulas were employed to consolidate the data into a single value for each study [11].
When there were x, y values or x, y, z values, the mean can be calculated using the following formula:
$$_\approx \sqrt_^+_^+_^}$$
When there were x, y values or x, y, z values, the standard deviation was obtained using the variance propagation formula.
$$_\approx \sqrt_}_}^_^+(\frac_}_}^_^}$$
$$_\approx \sqrt_^._^+_^._^+_^._^}_^}}$$
In the presence of multiple reference points, the average value was obtained using the arithmetic mean formula:
$$\mu =\frac\left(_+_+\dots +_\right)$$
In the presence of multiple reference points, the standard deviation was calculated using the pooled standard deviation.
$$_}=\sqrt_-1\right)_^+\left(_-1\right)_^+\dots +\left(_-1\right)_^}_+_+\dots +_-k}}$$
In cases where x, y values or x, y, z values were provided from multiple reference points, the three-dimensional values were calculated, considering the presence of these multiple reference points to determine the final value.
When sample size, median, range, and/or interquartile range or minimum and maximum values were available, the sample mean and standard deviation were estimated and calculated accordingly [11]. Data were analyzed using RevMan software (The Cochrane Collaboration, Copenhagen, Denmark), employing a random-effects model with inverse variance weighting to estimate the mean differences, along with 95% confidence intervals (CIs). Heterogeneity among the studies was assessed using statistical measures including Tau-squared (τ2), chi-squared (χ2) tests, degrees of freedom (df), and the I2 statistic. To further explore the meta-analysis results, we conducted a sensitivity analysis by sequentially removing each study to evaluate its impact on the overall findings. This approach allowed us to determine the robustness of the results and assess the potential influence of any single study on the overall effect estimates.
留言 (0)