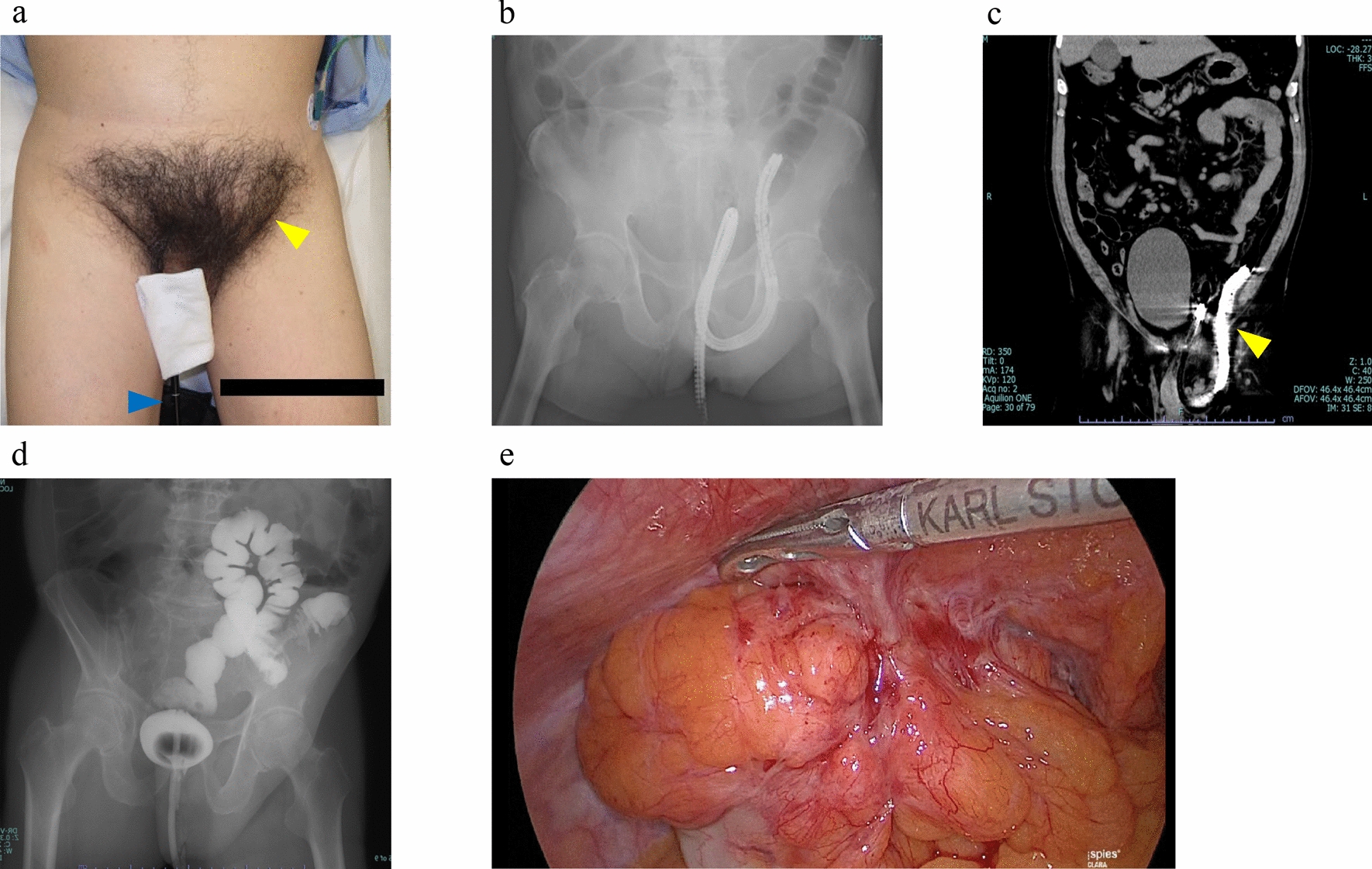
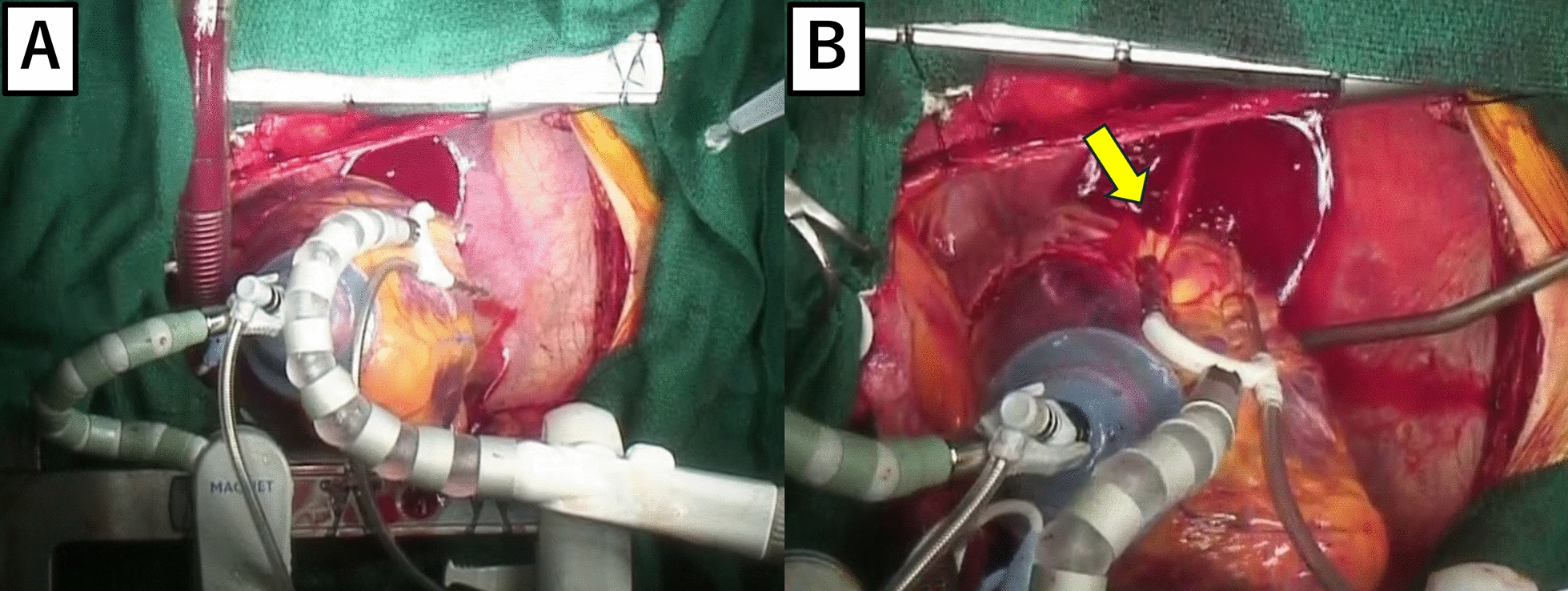
IHs are classified into congenital and acquired. In most cases, the defect is congenital. This phenomenon is attributed to two reasons: first, IH can develop in a wide range of ages. However, in most cases, it occurs in children. Second, based on intraoperative findings, the defect is usually circular and smooth, and it lacks signs of inflammation. In our case, although the mechanism of formation was unclear, he had no history of abdominal trauma, and the defect’s edges were smooth. In addition, the development of the marginal vessels indicates that the defect enlarged and that it had a chronic course. Hence, the patient’s mesenteric hiatal hernia could be congenital.
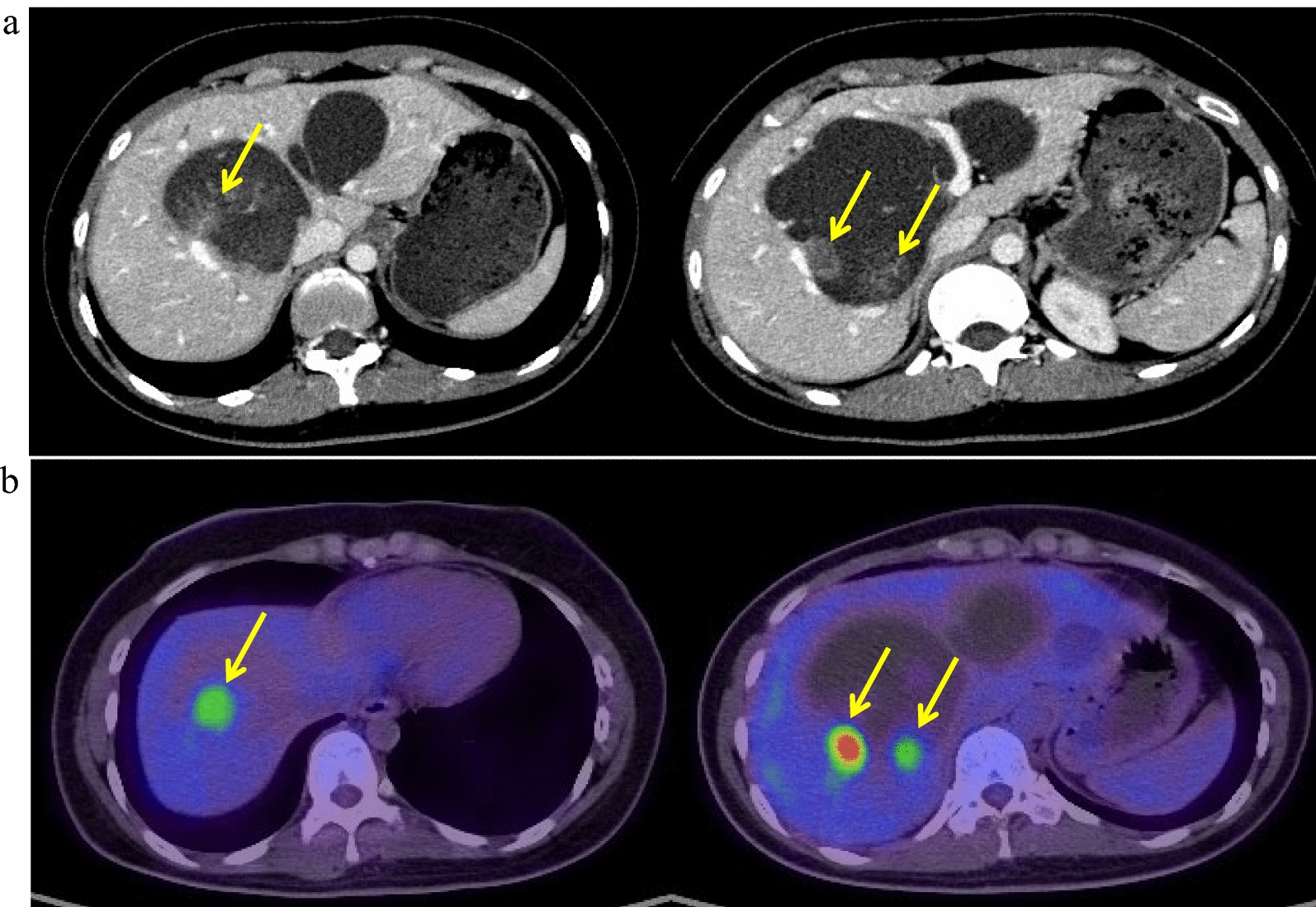
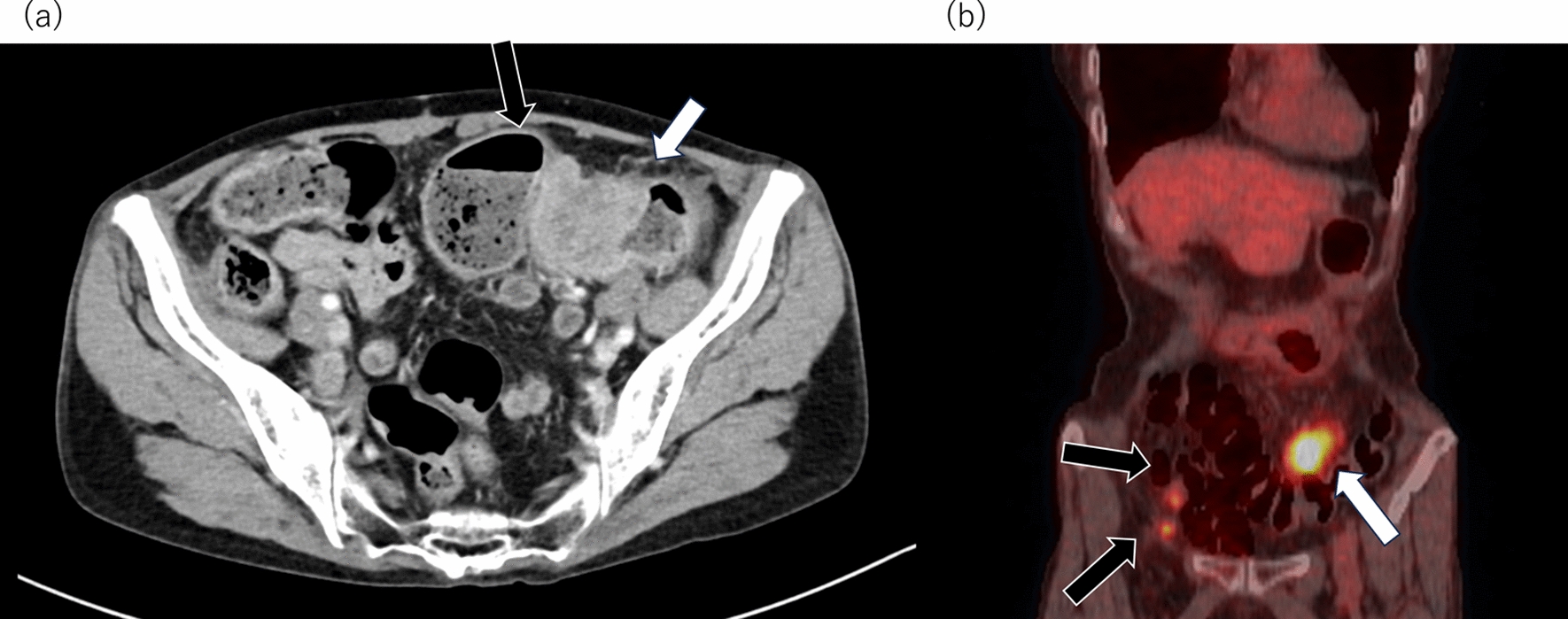
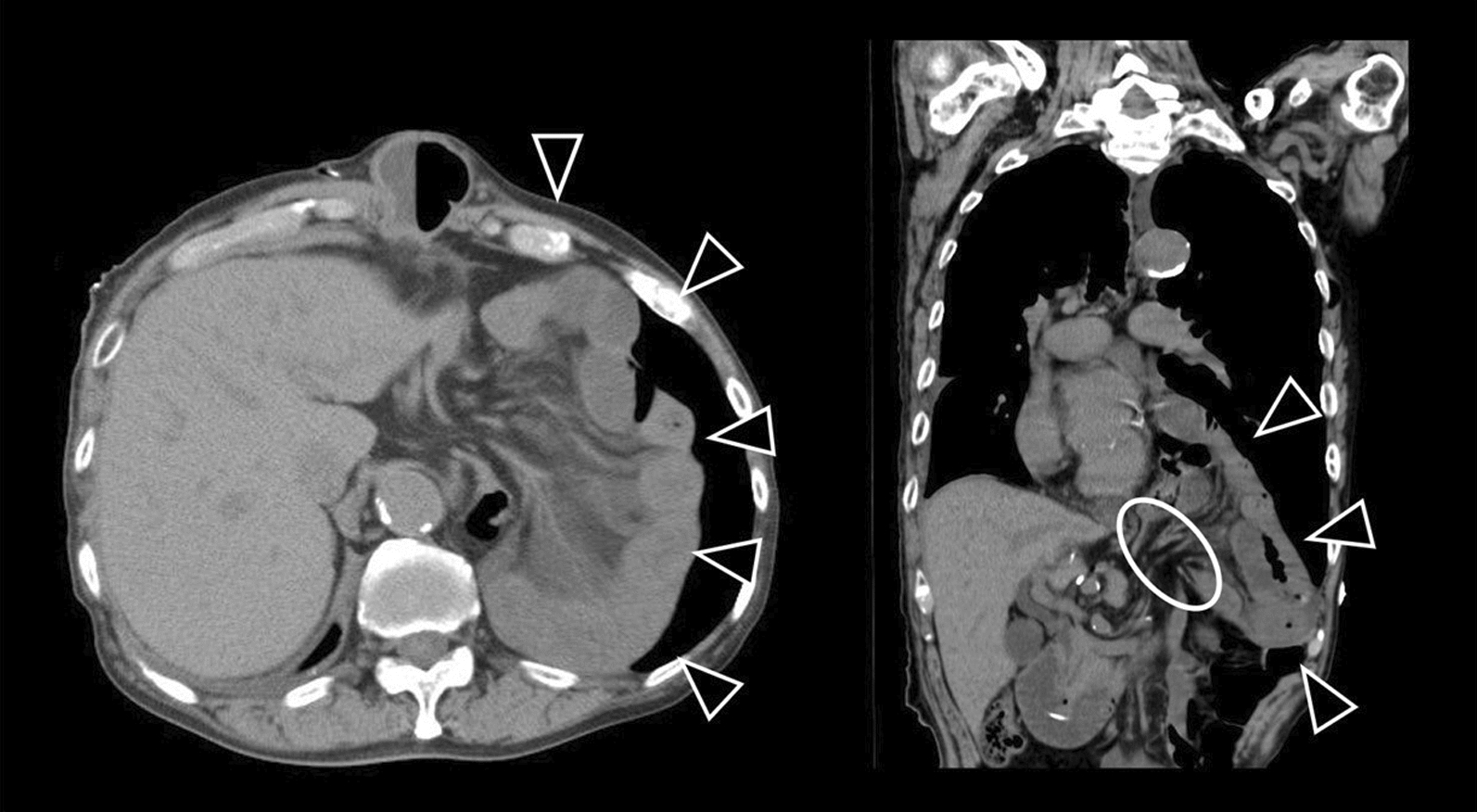
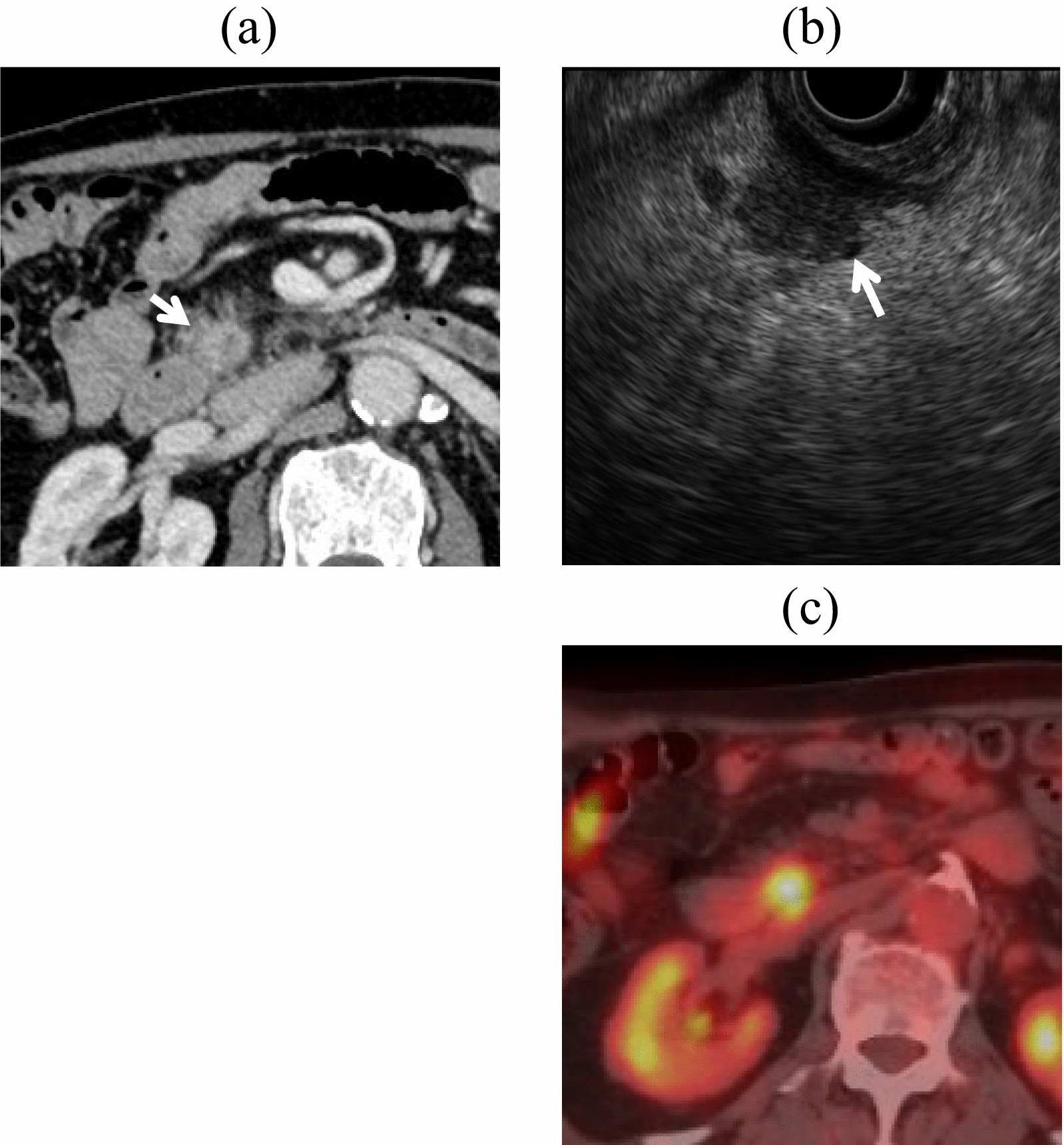
SMHH is challenging to diagnose preoperatively. Blachar et al. showed that the characteristic CT scan findings of SMHH include a closed loop in the small intestine, clustered and congested mesenteric vessels, and displacement of the mesenteric vascular trunk [6]. In our case, the patient presented with a closed loop pattern, and strangulated intestinal obstruction caused by the internal hernia was suspected. However, the actual cause was not identified preoperatively. This emphasizes diagnostic difficulties in this condition without specific considerations.
Although there are a few documented and published case reports, systematic reviews on the presentation, ideal management, and outcomes of IH are not available. A search for studies on small mesenteric hiatus hernias from 1983 to 2023, which excluded conference proceedings, revealed 29 adult (aged 20 years and older) cases in Japan [4, 7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32] (Table 2). The mean age of the patients was 48.9 years, and sex differences were not observed. The ileal mesentery is the most common site, and the average defect size was 6.8 (standard deviation: 6.2) cm. The defect in our case was significantly larger than that in other cases. Although there is no specific definition for large-diameter SMHHs, a defect greater than 15 cm was only observed in four cases. According to Ohata et al., the median defect size in pediatric cases is < 4 cm, which is smaller than the average defect size in adults [7]. Therefore, if the mesenteric hiatal defect is large, the patient can avoid strangulated intestinal obstruction in childhood.
Table 2 Adult cases of small mesenteric hiatal herniaThe surgical techniques for IHs associated with an abnormal hiatus include necrotic bowel resection and defect closure for hernial repair. If bowel necrosis is suspected, bowel resection is required. Hori et al. reported that different surgical techniques can be used for SMHHs [4]. In particular, 102 (76.7%) of 133 patients with SMHHs underwent bowel resection, and 31 (23.2%) patients did not. Further, 63 patients received surgical treatment for an abnormal defect. The defect was resected in 41 (65.1%) cases, and suture closure for defect repair was performed on 22 (34.9%) patients [4]. If the hernia defect is large, suture closure could be beneficial to preserve the margin artery and shorten the length of the bowel that should be resected.





留言 (0)