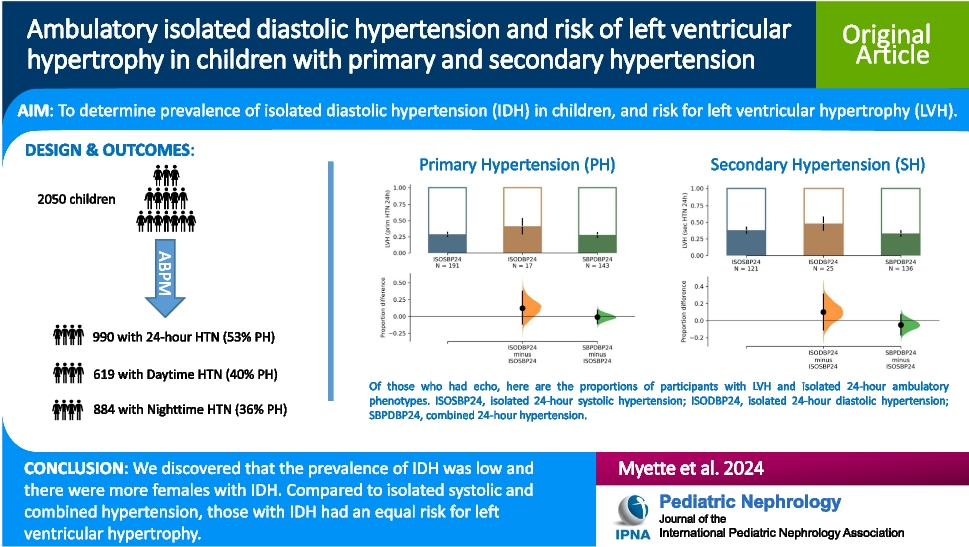
The key findings in our study include the observation of a varying prevalence of IDH across ABP phenotypes (6–12%). There was a lower prevalence of IDH in those with PH (6–8%), but a higher prevalence of IDH in children with SH (11–12%). Further, we observed differences in the prevalence of IDH because of biological sex, noting that females tended to have IDH more than males. Importantly, we also saw that the risk of LVH in our cohort was similar across all ABP phenotypes.
Our results agree with Rasała et al. [6], who observed higher DBP loads and levels in patients with SH using ABPM. We similarly observed a higher prevalence of ambulatory IDH in those with SH. Alsaeed et al. observed a similar low prevalence of IDH [5]; however, they used NHANES office data.
Knowing that differences in prevalence of hypertension based on sex have been described in the literature, we next sought to determine if there were sex-related prevalence differences between the ABP phenotypes, and specifically IDH, in our cohort. When further considering the observations of Alsaeed et al., [5] whereby they reported on an IDH phenotype using office BP measurements (more likely female, leaner, lower BMI), our study adds value in that we also observed this for those children with 24-h hypertension and both PH and SH. When comparing those with daytime hypertension and PH, there were more females with SDH; however, this was not the case for those with SH where children with IDH were again more likely to be female, like our observations for those with 24-h hypertension. There did not appear to be a sex predilection when comparing across ABP phenotypes and nighttime PH or SH. Intriguingly, the opposite was seen in Ali et al.’s study [14], and in a large study of Chinese adults, with more men having IDH [15].
It appears that not only is sex a possible factor but also age appears to be important. Alsaeed et al. [5] also observed that children with IDH tended to be younger. We did not observe that children with 24-h IDH, or daytime IDH were younger. However, those with nighttime IDH and either PH or SH were younger than those with ISH (P < 0.05).
Most importantly, a key finding from our study is that children with IDH on ABPM (either 24-h, daytime, or nighttime) had similar LVMI, aLVMI, and prevalence of LVH to those with ISH and SDH. This contrasts with the existing literature. The impact of increased blood pressure on HMOD in children with PH was assessed by Hamdani et al. [16], where they evaluated HMOD in participants who had ABPM and echocardiography within weeks of one another and concluded that DBP had no additive value in the prediction of LVH [16]. Other pediatric studies have looked at DBP and identified this to be non-consequential for LVH or HMOD [4, 17]. Specifically, Obrycki et al. studied ~ 300 pediatric patients with PH, assessing the impact of pre-hypertension on HMOD [4] and observed that 24-h DBP was not a predictor of negative changes in pulse wave velocity (PWV) or carotid intima-media thickness (cIMT), nor LVH [4]. Our results may differ owing to a larger sample size with a wider range of ages enrolled in this cohort.
While it requires further investigation, it would appear that IDH has an impact on LVH in both PH and SH and as such may have treatment implications. Drawing on literature from adult patients, it is clear that physicians have differing views on the importance of IDH with respect to HMOD and cardiovascular risk [18, 19]. One of the important takeaways from recent literature was the apparent increased risk for young patients with IDH. Indeed, in a study by Lee et al., those young adult patients (20–39 years old) whose BP category was Stage I diastolic hypertension had an increased estimated hazard ratio (HR) for cardiovascular disease (CVD) events and those with Stage II diastolic hypertension had an even higher risk [19, 20]. However, it is unclear whether these patients had PH or SH. Furthermore, when assessing the impact of BP change on risk of CVD events, Lee et al. were also able to show that by reducing DBP from Stage I hypertension to normotension, patients had a lower risk of CVD events compared to those that maintained Stage I [20]. Contrary to this, Jacobsen [21] argued in a recent adult cohort study and meta-analysis that isolated diastolic hypertension only appears to be important in those with controlled systolic hypertension and a DBP > 90 mmHg. He also argued that when using the AHA definition of IDH, there were no consistent, statistically significant associations with coronary artery calcification or incident cardiovascular events. However, they concluded that further studies in younger adults (and thus in children and adolescents) to better understand the risk of IDH were required.
The strengths of our study include the international, multicenter nature allowing for representation from multiple countries. Further, to our knowledge, this is one of the largest studies addressing ambulatory isolated diastolic hypertension with echocardiographic data in children. However, our study is not without limitations which are mainly the result of the retrospective design. We were unable to have our echocardiographic data validated by an independent examiner. Another limitation includes the inherent accuracy issues with oscillometric DBP measurements. Further, in some instances, the timing between ABPM and echocardiography was longer than 6 months (~ 10%); however, we reanalyzed the data using a strict 6-month cutoff between ABPM and echocardiography and the overall message was the same: the risk of LVH was no different between those with ISH, SDH, or IDH. Another limitation is the modification of guidelines around which patient should have an echocardiogram (across the 10-year enrollment period). We also did not assess for the impact of race, as this was not a variable reliably collected from all centers. Lastly, some children were treated for their hypertension, while others were not, or the data are not available. Future prospective studies are required to fully delineate the impact of IDH on LVH in children and adolescents.
In summary, we have analyzed data from a large, multi-center, international cohort of children, with ABPM and echocardiogram. To our knowledge, this is one of the largest cohorts of pediatric patients with nearly complete data allowing for direct comparison of ABP phenotypes, between those with PH and SH, to aLVMI. Our key findings were that ambulatory IDH was observed in ~ 10% of all patients in this cohort, there were more females with IDH, and children with ambulatory IDH, regardless of PH or SH, had essentially equal LVMI, aLVMI, and LVH risk. Although some studies have shown no strong association between DBP and LVH, our study shows that children with IDH have a similar prevalence of LVH when compared to ISH and SDH.





留言 (0)