
記住我




After exclusions (missing uNGAL and missing SCr [n = 115]), 476 children were included in the analysis (Supplemental Fig. 1). Median age (IQR) among them was 4.77 (1.43–30.40) months. Four hundred forty-four patients (94%) underwent CPB, 151 (32%) had single ventricle status, and there were 23 (4.8%) deaths. The median (IQR) number of ventilator-free days was 27 (25, 28) and ICU-free days was 23 (15, 26).
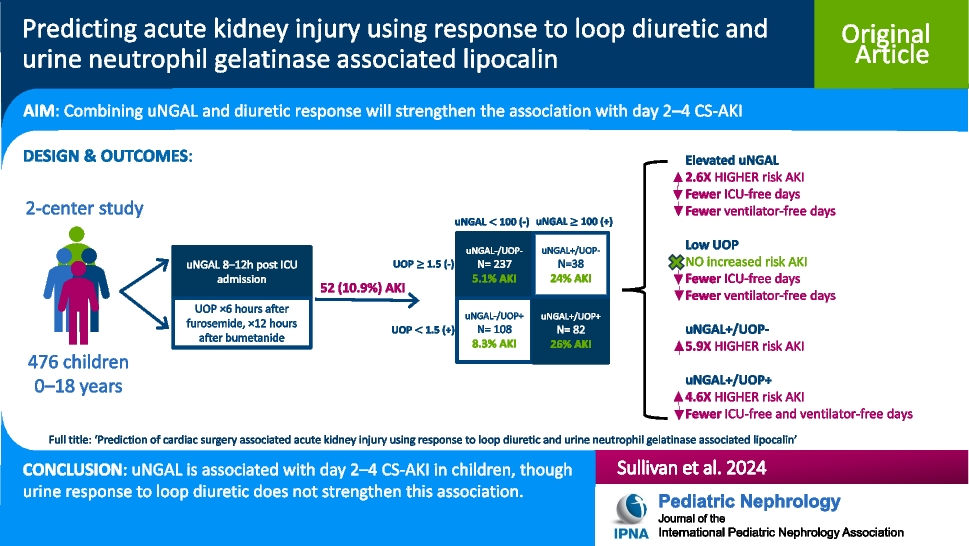
Postoperative day 2–4 CS-AKI associationsFifty-two (10.9%) patients developed day 2–4 CS-AKI (Supplemental Fig. 1), of which 32 (6.7%) were classified as severe (stage 2 or 3) and 11 (2.3%) received KRT. Table 1 summarizes the demographics, clinical features, and outcomes of patients with day 2–4 CS-AKI compared to those without. There was no difference in age (as a continuous variable) and sex among patients with and without day 2–4 CS-AKI. There was no difference in furosemide dose equivalents indexed to weight between groups. Patients with day 2–4 CS-AKI had higher surgical complexity as evidenced by a higher proportion of STAT 4 or 5 operations, more frequent single ventricle heart disease (46% vs. 30%), and longer CPB duration (180 min, [IQR: 123–284] vs. 146 min [IQR: 105–197] compared to those with no day 2–4 CS-AKI (p = 0.007, p = 0.027, and p = 0.006 respectively). Patients with day 2–4 CS-AKI had a higher severity of illness as measured by vasoactive inotrope score at 8 h after CICU admission (p = 0.005). Patients with day 2–4 CS-AKI had a median of 1 less ventilator-free day and 8 less ICU-free days compared to those without day 2–4 CS-AKI (p = 0.018 and p < 0.001 respectively). Mortality was 4 times higher among patients with day 2–4 CS-AKI compared to no day 2–4 CS-AKI (15% vs. 3.5%, p < 0.001).
Table 1 Demographics, clinical features, and outcomes of those with and without AKILoop diuretic comparisonsFurosemide was the most common diuretic used in 60% (n = 281). Supplemental Table 2 compares the demographics, clinical features and outcomes of those who received bumetanide vs. furosemide. Those who received bumetanide were younger, underwent more complex surgeries and were sicker than those who received furosemide. Day 2–4 CS-AKI occurred in 16% (n = 30) of those who received bumetanide and 7.5% (n = 21) of those who received furosemide (p = 0.005). There was no difference in mortality between groups, but those exposed to bumetanide had fewer ventilator and ICU-free days.
Associations of continuous UOP response and uNGAL with postoperative day 2–4 CS-AKIPatients with day 2–4 CS-AKI had higher uNGAL (214.50 [IQR: 21.73–496.25] vs. 24.30 [10.00–76.62]; p < 0.001) and lower indexed UOP in response to loop diuretic (1.10 [0.46–2.54] vs. 2.10 [1.03–3.75]; p < 0.001). In multivariable logistic regression, uNGAL modeled as a continuous variable was associated with 2.59 greater odds of day 2–4 CS-AKI when comparing a value of 110.5 ng/mL (75th percentile) to a value of 10.0 ng/mL (25th percentile), IQ OR: 2.59 [1.52–4.41]) (Figs. 1, and 2B). Indexed UOP alone was not associated with day 2–4 CS-AKI (OR: 0.65 [0.30–1.41]) (Fig. 1). The predicted probabilities for day 2–4 CS-AKI when modeled as a non-linear function of uNGAL and UOP are presented in Fig. 2. The interaction term of uNGAL and UOP on the risk of day 2–4 CS-AKI was not significant (LRT chi-square = 1.88, degree of freedom [df] = 3, p = 0.597, Supplemental Table 3).
Fig. 1
Forest plot of predictors of day 2–4 acute kidney injury (AKI). Odds ratio (OR) and 95% confidence interval (CI) from a multivariable logistic regression model. For continuous variables, ORs were rescaled to reflect an increase from the first (25th percentile) to the third quartile (75th percentile). STAT: Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery, CBP: cardiopulmonary bypass, uNGAL: urine neutrophil gelatinase associated lipocalin
Fig. 2
Probability of day 2–4 acute kidney injury (AKI) as a function of indexed urine output (A) and urine neutrophil gelatinase associated lipocalin (uNGAL) (B) from multivariable logistic regression, adjusted for a priori relevant covariates at the most frequent or median level. Indexed urine output and uNGAL were modeled with restricted cubic splines (3 knots) to allow for potential non-linear association with day 2–4 any AKI. Shaded area denotes 95% confidence intervals
We compared uNGAL alone and UOP alone for prediction of day 2–4 CS-AKI using univariate receiver operating curve analysis. The area under the receiver operating curve (AUC) using a priori cutoffs for uNGAL and UOP for predicting day 2–4 CS-AKI was 0.69 and 0.60, respectively (Fig. 3A). We then sought to determine the most optimal cutoffs for uNGAL and UOP based on Youden’s index. The optimal cutoff for uNGAL was ≥ 127 ng/mL and for UOP was ≤ 0.79 mL/kg/hr. The AUC for each was 0.70 and 0.65, respectively, for predicting day 2–4 CS-AKI (Fig. 3B). The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) using both the a priori and optimal cutoffs are summarized in Supplemental Table 4.
Fig. 3
Observed receiver operating curves for prediction of day 2–4 AKI using a priori cutoffs (A) vs optimal cutoffs defined by Youden’s index (B). Area under the receiving operator curve (AUC) for prediction of postoperative day 2–4 AKI using uNGAL ≥ 100 ng/mL alone, UOP < 1.5 mL/kg/h alone, and UOP < 1.5 mL/kg/h + uNGAL ≥ 100 ng/mL (A). AUC for prediction of postoperative day 2–4 AKI using uNGAL ≥ 127 ng/mL alone, UOP ≤ 0.79 mL/kg/h alone, and UOP ≤ 0.79 mL/kg/h + NGAL ≥ 127 ng/mL (B). UOP: urine output, uNGAL: urine neutrophil gelatinase associated lipocalin
Comparing c-statistics of multivariable logistic regression, the models with uNGAL alone, uNGAL + UOP, and uNGAL + UOP + their interaction had similar performance for prediction of day 2–4 CS-AKI (optimism-corrected c-statistics: 0.744 vs. 0.737 vs. 0.722) (Supplemental Table 3). The adequacy index comparing likelihood ratios for the model with uNGAL only to that with uNGAL + UOP was 0.966. UOP adds only a fraction of 0.034 of new predictive information to uNGAL. The model LRT shows that the addition of UOP to uNGAL did not significantly improve discrimination for predicting day 2–4 CS-AKI (LRT chi-square = 1.65, df = 2, p = 0.439) (Supplemental Table 4).
Because of the non-linear relationship between uNGAL and UOP with day 2–4 CS-AKI, we assessed the probability of day 2–4 CS-AKI for each predictor individually but stratified by the other (Fig. 2). The probability of day 2–4 CS-AKI increases with lower UOP when stratified by uNGAL concentration (Fig. 2A). There was a decrease in UOP with higher thresholds of uNGAL. The probability of day 2–4 CS-AKI also increases with increasing uNGAL at different thresholds of UOP (Fig. 2B). There was a significant increase in uNGAL with lower thresholds of UOP.
Associations with secondary outcomesIn multivariable analysis, higher uNGAL was associated with fewer ventilator-free (IQR OR: 0.59, 95%CI: 0.44–0.79) and fewer ICU-free days (IQR OR: 0.72, 95%CI: 0.53–0.96) (Supplemental Fig. 2A, B). uNGAL was not associated with mortality (IQR OR: 1.46, 95%CI: 0.65–3.29) (Supplemental Fig. 2C). Higher indexed UOP was associated with more ventilator-free (IQR OR: 3.51, 95%CI: 2.31–5.33) and more ICU-free (IQR OR: 2.09, 95%CI: 1.38–3.15) days (Supplemental Fig. 2D, E), but not mortality (IQR OR: 0.80, 95%CI: 0.23–2.72) (Supplemental Fig. 2F).
Sub-phenotypes of uNGAL and urine outputOf the 4 sub-phenotypes (Supplemental Fig. 3): 237 patients (51%) uNGAL–/UOP–, 108 (23%) uNGAL–/UOP + , 38 (8%) uNGAL + /UOP–, and 82 (18%) uNGAL + /UOP + . Demographics, clinical characteristics and outcomes for the sub-phenotypes are summarized in Table 2. Those with uNGAL + /UOP + were significantly younger than all other sub-phenotypes with a median (IQR) age of 0.38 months (0.20, 3.17) and 91% (n = 75) being < 1 year (p < 0.001). There were also significant differences in intraoperative and postoperative characteristics across sub-phenotypes, with those with uNGAL + /UOP + having the highest surgical complexity, longer circulatory arrest, increased utilization of delayed sternal closure and higher vasoactive inotrope score at 8 h as compared to other sub-phenotypes (Table 2).
Table 2 Demographics, clinical features, and outcomes across the 4 sub-phenotypesAssociations of uNGAL and UOP sub-phenotypes with postoperative day 2–4 CS-AKIThe frequency of day 2–4 CS-AKI was highest among the uNGAL + /UOP + sub-phenotype (26%, n = 21) followed by uNGAL + /UOP– (24%, n = 9) (p < 0.001). In multivariable logistic regression, both uNGAL + /UOP + (IQR OR: 4.63, 95%CI: 0.65–3.29) and uNGAL + /UOP– (IQR OR: 5.94, 95%CI: 2.09–16.84) were associated with day 2–4 CS-AKI when compared with uNGAL–/UOP–, after adjusting for covariates (Fig. 4). The test characteristics (sensitivity, specificity, PPV and NPV) for each of the sub-phenotypes using the a priori cutoffs and the optimal cutoffs are summarized in Supplemental Table 4. Using the optimal cutoffs (uNGAL ≥ 127 and UOP ≤ 0.79), the AUC for uNGAL + /UOP + improved from 0.67 to 0.75 (Fig. 3).
Fig. 4
Forest plot of sub-phenotypes as predictors of day 2–4 AKI. Odds ratio (OR) and 95% confidence interval (CI) from a multivariable logistic regression model including the predictors listed in the figure. For continuous variables, ORs were rescaled to reflect an increase from the first (25th percentile) to the third quartile (75th percentile). Both uNGAL + /UOP + and uNGAL + /UOP– are associated with day 2–4 AKI when compared with uNGAL–/UOP–
Associations of uNGAL and UOP sub-phenotypes with secondary outcomesThe uNGAL + /UOP + sub-phenotype had the fewest ventilator-free days (24, IQR: 20–26) (p < 0.001). The uNGAL + /UOP + sub-phenotype had the fewest ICU-free days (13, IQR: 2–20) followed by the uNGAL + /UOP– group (19, IQR: 7–25) (p < 0.001). Mortality was significantly higher in those with uNGAL + /UOP + as compared to all the other sub-phenotypes (p < 0.001).
When compared with the uNGAL–/UOP– sub-phenotype using logistic regression and ordinal regression models, the uNGAL + /UOP + group had fewer ventilator-free days (OR: 0.17, 95%CI: 0.10–0.29) and fewer ICU-free days (OR: 0.31, 95%CI: 0.18–0.53) (Supplemental Fig. 4). There was no association of uNGAL + /UOP + with mortality (OR:3.25, 95%CI: 0.74–14.33) (Supplemental Fig. 4).
留言 (0)