
記住我

A cohort of n = 50 (n = 30 male, n = 20 female) experienced cyclists with more than three years of regular cycling exercise (> 2 sessions per week) were recruited for this study. All participants were experienced in road cycling with clipless pedals and cycled regularly as exercise. Prior to the study, the participants were informed of the protocol and gave their written informed consent to participate. All procedures were approved by the ethical committee of Exercise Science & Training of the Faculty of Human Sciences of the University of Würzburg (EV2024/1-1004) and conducted in accordance with the Declaration of Helsinki (Harriss and Atkinson 2009; World Medical Association 2013). Characteristics of participants are given in Table 1.
Table 1 Mean ± SD of age, body stature, selected anthropometric data and peak oxygen uptake of participants obtained during the first visitExperimental designThree experimental visits to the laboratory were required which were at least 48 h apart and completed within a period of two weeks. The first visit was to familiarize participants with the all-out sprint and determine their \(}}\)O2peak in a ramp test. Figure 1 illustrates the timeline and all testing procedure for each visit.
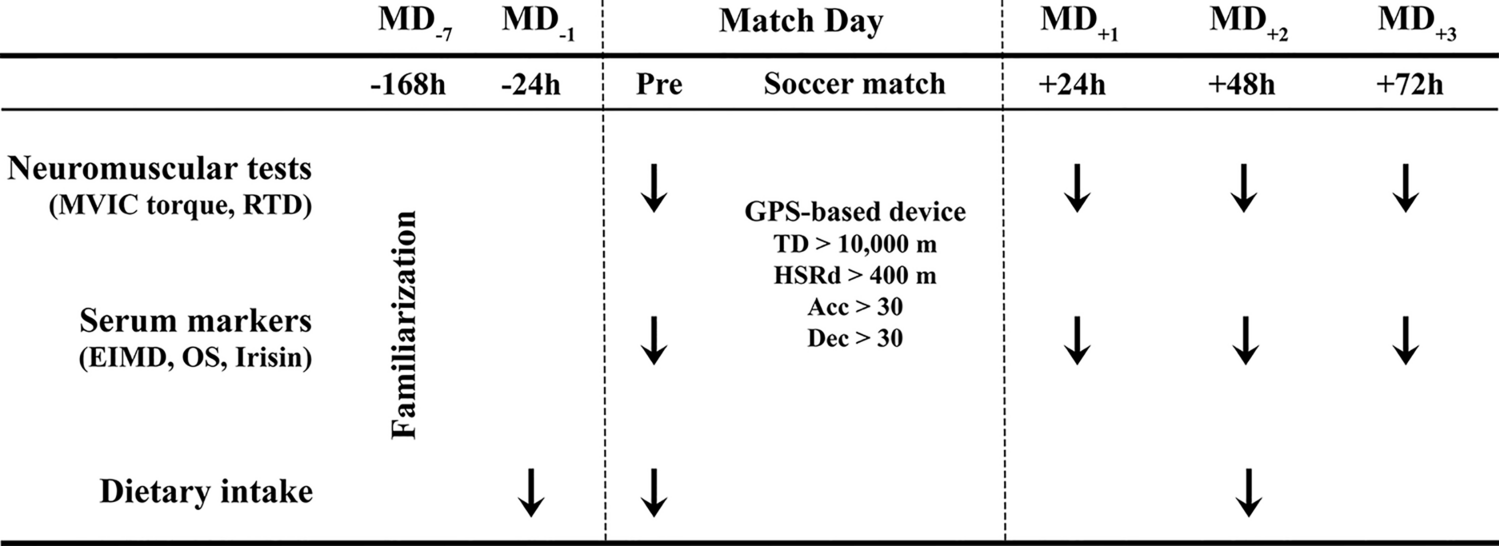
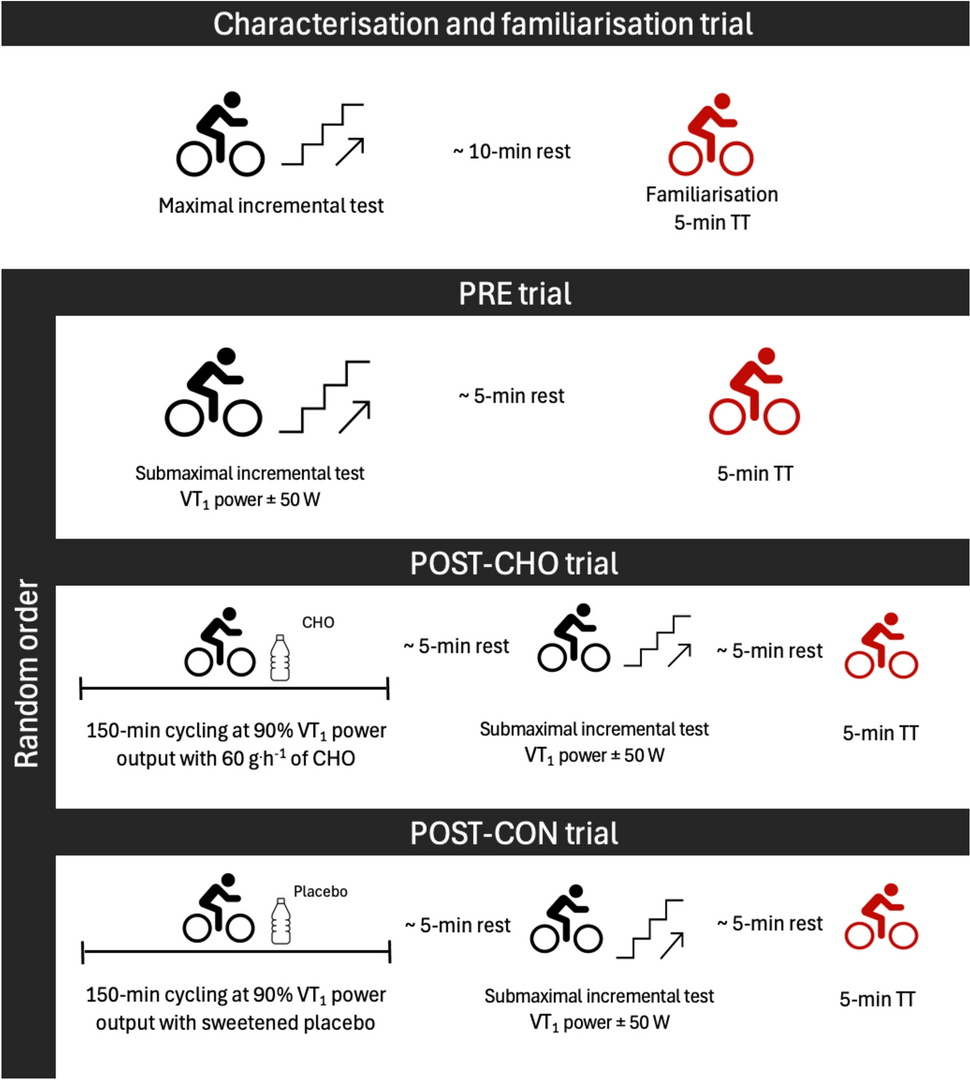
Fig. 1
Illustration of the timeline of all study procedures
All participants were instructed to keep a nutrition diary and to repeat their usual diet for each visit within the 24 h before each experimental visit (Jeacocke and Burke 2010). In addition, all were instructed to stay adequately hydrated, to eat a carbohydrate-rich meal (i.e., a banana and a jam sandwich) no less than 3 h before each visit and to refrain from caffeine consumption on the day. Each participant received 35 g of a carbohydrate mixture (IsoFast, DextroEnergy, Krefeld, Germany) dissolved in 500 ml of water to drink ad libitum during warm-up and recovery periods. All participants provided a urine sample in a cup first when visiting the laboratory. Hydration status was then promptly tested via urine specific gravity analysis employing a dipstick (One step 10, DFI Co., Gyeongsangnam-do, South Korea).
During the first visit (T1), body composition (i.e., FFM) of all participants was measured employing eight-electrode impedance analysis (InBody 720, Biospace, Des Moines, Iowa, USA). During the second (T2) and third (T3) visit, only a warm-up and 15-s all-out cycle sprint test were performed.
All 15-s all-out cycle sprints were conducted on their own personal road bike installed on a Cyclus2 ergometer (RBM, Leipzig, Germany). The Cyclus2 is an electromagnetically braked ergometer and measures power with an accuracy error of 2% according to the manufacturer. All cyclists used their own shoes and pedals for all tests. For all three visits, all cyclists warmed up for 10 min cycling at 1.5 W/kg body mass and resting for 3 min (Quittmann et al. 2021a, b).
The all-out cycle sprint was performed in a seated position utilizing the large chainring (if applicable) of the participant’s bike and the 15-tooth cog of the ergometer. Recording of the test started with cadence of > 30 RPM. The ergometer software was set to isokinetic mode and 130 RPM (Adam et al. 2015; Nitzsche, et al. 2018; Quittmann et al. 2020; Quittmann et al. 2021a, b).
Capillary blood samples of the left earlobe were sampled twice during the resting period, directly after the warm-up while resting passively and once directly after the sprint as well as every minute for 8 minutes after the 15 s cycle sprint. Lactate concentration was measured amperometric-enzymatically employing Biosen C-Line (EKF Diagnostics, Barleben, Germany). Peak lactate was taken as the highest measured concentration during the passive rest period. ∆La was calculated as the difference between the average of resting values (Lapre) and the peak values attained in the post-exercise resting period (Lapeakpost).
Approximately 30 min after the sprint test, V̇̇O2peak was determined in a ramp test protocol. Participants were fitted with a Hans Rudolph V2 mask (Hans Rudolph, Inc, Shawnee, KS, USA) and expired gasses and breathing volume were analyzed with Cosmed Quark CPET (Cosmed Srl, Rome, Italy). The gas and volume analyzers were calibrated before every test with precision gas (16% O2; 5% CO2) and a volume pump in accordance with the manufacturer's instructions (Airgas Therapeutics, Plumsteadville, PA, USA). Participants cycled at 100 W for 2 min with freely chosen cadence. Thereafter the load increased by 25 W every 30 s (Adam et al. 2015). The test ended when volitional exhaustion was reached or cadence dropped by more than 10 RPM. V̇O2peak was calculated as the highest value averaged over 30 s.
Mechanical energy equivalent of lactateAs result of the previously shown high reliability of the testing procedure for 15 s-work (ICC = 0.99) and ∆La (ICC = 0.91), 15 s-work and ∆La was averaged from T2 and T3 to account for day-to-day variability (Zinner et al. 2023; Meixner et al. 2024). T1 was considered as familiarization because of decreased reliability compared to T2 and T3.
The calculation of glycolytic energy contribution was based on previous work (Margaria et al. 1963, 1964). An oxygen equivalent of 3 ml O2 per kg bodyweight was assumed per 1 mmol/l of accumulated lactate in capillary blood blood. This oxygen equivalent was transformed to work assuming an energy equivalent of 21.1 kJ/l O2 and gross efficiency of 20% (Scott 2005).
As total body water is a constant in humans of 73% of FFM (Wang et al. 1999) and Mader and Heck consider 69% of total body water to be available as lactate-distribution space (Mader and Heck 1986), lactate-distribution space is ≈ 0.5*FFM. In the present study, an equivalent measure to the method of Margaria was calculated multiplying ΔLa with lactate-distribution space as assumed total lactate production. An oxygen equivalent of 7 ml O2 per kg FFM per change of mol of capillary blood lactate accumulated was determined to be comparable to the method of Margaria via linear regression. The resulting value is referred to as glycolytic energy contribution.
Considering the apparent influence of FFM and total lactate production, we conducted a post-hoc analysis to identify all possible pairs of participants whose FFM differed by no more than 1.5%. For these pairs (n = 51), the impact of FFM on differences in 15 s-work output was deemed negligible. Subsequently, we calculated the mechanical energy equivalent of blood-lactate accumulation by relating the difference in relative 15 s-work per kilogram of FFM between pairs to the difference in ΔLa for each pair.
Statistical analysesRaw data was processed using Microsoft Excel. Statistical analyses (mean, standard deviations, and 95% confidence intervals) were computed with GraphPad Prism (v10.2, Boston, MA, USA). Data normality for body mass, FFM, 15 s-work (absolute and relative to FFM) and ΔLa was assessed using the Kolmogorov–Smirnov test, Shapiro–Wilk test and visual inspection, without requiring further transformation. Level of significance (α) was set to 0.05 for all statistical analysis. Relations between 15 s-work, ΔLa, FFM and associated measures were analyzed employing simple and multiple linear regression models. Differences between males and females were analyzed by independent sample student t tests.
留言 (0)