Although SPN is potentially malignant, 95% of patients are disease-free after surgical resection, and the mortality rate is less than 2%, indicating a good prognosis [3].
SPN with duodenal invasion is rare. Papaviramidis et al. reported that 497 patients with SPN had evidence of metastasis or invasion; 97 were positive with 27, 26, 17, and 27 in the liver, portal vein, spleen, and other organs including the duodenum, respectively [4]. Zhan et al. reported 91 cases of SPN, with 1 case (1.1%) of duodenal invasion [5]. Natsume et al. reported a case of SPN ruptured into the duodenum requiring PD [6]. Ours is the first report on resecting an SPN invading the duodenum using pancreatic enucleation and partial duodenectomy.
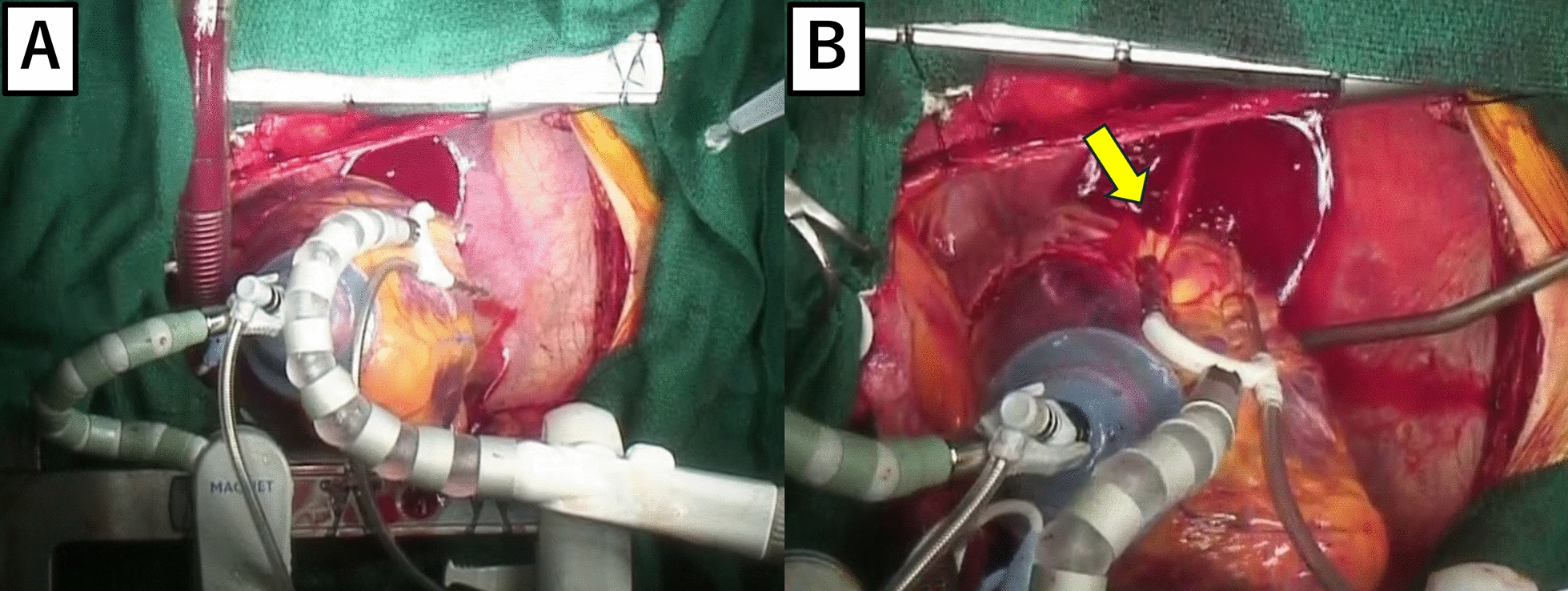
Although enucleation has been commonly performed for SPN of the pancreatic head recently, reports suggest that radical resection, including PD, should be performed in cases with local invasion or distant metastases [5]. But PD alters natural food passage leading to the mixing of oral nutrition with digestive enzymes, and the incidence of diabetes mellitus after surgery is 15–40%, pathologic exocrine pancreatic function varied from 22 to 55% due to the loss of healthy pancreatic parenchyma [7]. Enucleation is a simple procedure with short surgical duration, low blood loss, and good maintenance of pancreatic endocrine/exocrine function [8]. Only 2% of patients with SPNs have lymph node metastases [3]. Considering that SPNs are often low-grade and rarely have lymph node metastases, enucleation with a low risk of pancreatic endocrine/ exocrine dysfunction shows significant benefits, especially in children, in whom PD may be over-invasive. In this patient, enucleation from the pancreas allowed tumor resection with minimal pancreatic parenchyma loss, and using endoscopy, the duodenal side of the tumor could be resected precisely, avoiding extensive resection with PD and excessive reconstruction with gastrointestinal pathway alteration. We believe that a reduction surgery like this one should be considered when the tumor is expected to be completely resectable and damage to surrounding organs is anticipated to be acceptable, even for duodenal invasion of SPN. Specifically, the tumor should be located on the periphery of the pancreatic head, the size should allow for enucleation with a low risk of injuring the main pancreatic duct, neither enlarged lymph nodes nor invaded major blood vessels should be evident, and when the duodenal diameter after tumor resection and suturing should not be expected to cause stenosis. Particular attention should be given to the possibility of tumor recurrence after reduction surgery. The median time to recurrence is reported to be 4 years [3], so in this case, follow-up is planned for over 5 years using a combination of abdominal ultrasound and MRI.
We considered endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) biopsy to confirm the diagnosis, but neoadjuvant chemotherapy has limited efficacy in the treatment of the suspected pediatric GIST [9], and the lesion would likely need to be resected to control the bleeding; therefore, primary surgery was selected. In a systematic review of 2744 patients with SPN, preoperative percutaneous or EUS-FNA biopsies were performed in 253 patients, and 64.8% were diagnostic of SPN [3]. EUS-FNA may be diagnostic, but its accuracy varies, and it is only recommended for unresectable cases [10]. In a US National Cancer Database study, biopsies were performed in 28.7% of pediatric patients with SPN [11]. Although preoperative biopsy is uncommon in children with suspected SPN, in this patient, tumor resection after pathological diagnosis may have avoided tumor capsule failure and prevented pancreatic fistula by identifying it as a pancreatic tumor, and allowing more careful dissection of the pancreatic side.





留言 (0)