This study provides important insights into temporal changes in medically certified sick leave and primary healthcare utilization in Norway, reflecting systemic changes in healthcare utilization and labor markets. Our findings indicate significant excesses in working person-days lost to medically certified sick leave and primary healthcare consultations in 2023, deviating from the 2010–2019 trends. Many of these changes were found to be temporally correlated with a proxy for community spread of COVID-19.
This is an observational study of aggregated temporal trends, so causal attribution of the findings is not possible. There have been several large changes to Norwegian society between 2020 and 2023, such as the wide-spread introduction of a novel virus (SARS-CoV-2), comprehensive preventative measures in 2020 and 2021, and the cost-of-living-crisis in 2022–2023. All of these may have served to exacerbate existing trends or create new trends. We shall therefore interpret with caution our findings that may be evidence of larger trends identified elsewhere.
The role of e-consultations in NorSySS
For the purposes of this study, both physical consultations and e-consultations were treated equally in NorSySS. The use of e-consultations in Norway grew dramatically from 2020, which could have affected our results by allowing for a lower-threshold to contact the general practitioner. From 2010 to 2019 the median of the mean annual number of consultations per general practitioner was 1957, with an IQR between 1947 and 1972. For 2020, 2021, 2022, and 2023, the mean annual number of consultations per general practitioner were 2028, 2122, 2047, and 1950 respectively. Given that the mean annual number of consultations per general practitioner in in 2023 had returned to the pre-pandemic norms, we consider it more likely that, in 2023, e-consultations had replaced physical consultations.
“Immunity debt”, “immunity theft”, and the impact of COVID-19
When considering the concept of “immunity debt”, it is important to note that any exposure to pathogens has an inherent risk of illness or death. Proposed by a group of French researchers, the concept argues that during the comprehensive measures in 2020 and 2021, newborn children were born into an environment with fewer circulating pathogens, hence not exposed to certain pathogens, resulting in them lacking adaptive immunity to these pathogens (compared to their equally aged counterfactuals in 2019) [23]. For some adolescents and adults, adaptive immunity for specific pathogens may have waned during 2020 and 2021. Consequently, when the comprehensive measures were lifted, the population without adaptive immunity to specific pathogens in 2022 was likely larger than in 2019. This suggests that, for a limited time, there would be a surge in some infectious diseases at the population level. This concept argues that exposure to various pathogens will gradually rebuild the population’s adaptive immunity to those pathogens (with an associated increase in illness and/or death for those exposed to the pathogens), eventually stabilizing infection rates to pre-pandemic levels. The concept does not support exposure to pathogens to improve adaptive immunity, as any exposure to pathogens has an inherent risk; vaccination is a safer method of gaining adaptive immunity to specific pathogens. The concept of “immunity debt” does not specify when the “debt” is expected be paid off.
COVID-19 is itself associated with subsequent increased risk of other diseases, which complicates the concept that “immunity debt” is the cause of increased illness after the cessation of comprehensive measures. This concept is known as “immunity theft,” where SARS-CoV-2 infection leaves some people more susceptible to other infections [24]. In support of “immunity theft”, one study in the US showed that COVID-19 was associated with a significantly increased risk of RSV among children aged 0–5 years in both 2022 and 2021, with the authors postulating that their findings “suggest that COVID-19 contributed to the 2022 surge of RSV cases in young children through the large buildup of COVID-19-infected children and the potential long-term adverse effects of COVID-19 on the immune and respiratory system” [25]. Another study found that, in Thailand, COVID-19 pneumonia was strongly associated with a higher hazard of detectable active pulmonary tuberculosis, and it was likely that this hazard was not fully explained by diagnostic bias [26].
For context, COVID-19 (suspected and confirmed) accounted for 56% and 19% of all respiratory-related lost working person-days to medically certified sick leave in Norway in 2022 and 2023, respectively (Table 3). In comparison, influenza accounted for 4% and 10% of these respiratory-related working person-days lost in the same years (Table 3).
Some post-acute sequelae of COVID-19, such as fatigue and respiratory issues, are similar to those of other post-viral illnesses, such as post-acute sequelae of influenza. However, the acute and post-acute burdens of COVID-19 are higher than influenza in a wide variety of organ systems [27]. Frequency of reinfection is a crucial driver of the incidence of post-viral illnesses; individuals are typically infected with influenza once every five years [28]. It is currently unknown how often an individual in Norway is reinfected with SARS-CoV-2.
In accordance with the Norwegian government’s COVID-19 strategy, risk assessments from the Norwegian Institute of Public Health do not consider the consequences of long-term sequelae; they instead focus solely on hospitalization, ICU-usage, and acute deaths [9].
This unique situation raises concerns about the long-term health impacts of repeated SARS-CoV-2 infections. Therefore, the discussion focuses on whether the literature supports that excess illness observed in 2023 could be partially or wholly attributed to acute sequelae of COVID-19, post-acute sequelae of COVID-19, or adverse effects on immune systems due to COVID-19.
Weakness/tiredness general (fatigue)
This study estimated an economic loss of 1.8 billion NOK / 161 million USD in 2023 due to excess working person-years lost to medically certified A04 (Weakness/tiredness general) sick leave.
Fatigue is one of the most well-known post-acute sequelae of COVID-19 [3]. A Norwegian study showed that people who tested positive for the Delta and Omicron variants of SARS-CoV-2 were more likely to seek healthcare for fatigue (the outcome included A04) in the 126 days post-infection compared to those who tested negative [14]. Another Norwegian study investigated if sickness absence due to COVID-19 was associated with subsequent sick leave due to A04 (Weakness/tiredness general) and found a strong positive association [29]. However, it is important to remember that A04 (Weakness/tiredness general) is a common diagnosis, and the increase may be partially or wholly explained by other causes than COVID-19; the use of the diagnosis has previously fluctuated with conditions in the labor market [30]. These studies indicate that the increase is likely to be associated with COVID-19, but other societal factors cannot be excluded.
The addition of all the deficits in 2023 (L81, N79, B99, K76, T85, T99, D87, R90, L71, D92) summed to negative 255,000 working person-days lost to medically certified sick leave. In comparison, A04’s excess was 660,000. Hence there is no evidence that A04’s excess can be fully explained by a change in coding practices.
If the increase in A04 is partially or wholly related to COVID-19, it could imply that the societal burden will continue to increase as new individuals are infected and develop long-lasting sequelae. A Danish study reported that more than 50% of patients at a post-COVID clinic showed no improvement after 1.5 years [6]. The diagnosis of A04 also corresponds to the diagnosis used for myalgic encephalomyelitis/chronic fatigue syndrome, of which about half of long-covid patients fulfill the criteria [31]. For this patient population, few show benefit of return-to-health/work interventions [32].
Psychological symptom/complaint other and depression
P29 (Psychological symptom/complaint other) accounts for 12% of the total excess working person-days lost to medically certified sick leave in 2023, for an estimated economic loss of 2 billion NOK / 177 million USD.
The ICPC-2 code P29 (Psychological symptom/complaint other) is used for psychological issues without an obvious source. For example, the Norwegian Directorate of Health’s (Norwegian: Helsedirektoratet) guidance to primary healthcare doctors regarding “burnout” is to record it under P29 [33].
A previous study by the Norwegian Labour and Welfare Administration analyzed all people on medically certified sick leave from 1st of January 2020 to 30th of June 2022 [29]. The study compared 253,460 people with medically certified sick leave due to COVID-19 against 718,328 people with medically certified sick leave for not COVID-19. The study found that within 0–30 days after the end of the medically certified sick leave, 533 people (210/100,000 people) in the COVID-19 group had a medically certified sick leave for P29, compared to 1475 people (205/100,000 people) in the non-COVID-19 group. Within 0–12 weeks, these numbers were 1410 people (556/100,000 people) in the COVID-19 group and 3392 people (472/100,000 people) in the non-COVID-19 group, corresponding to an 18% higher rate in the COVID-19 group. These numbers are not adjusted for confounders.
P03 (Feeling depressed) accounts for 5% of the total excess working person-days lost to medically certified sick leave in 2023, for an estimated economic loss of 740 million NOK / 67 million USD.
In 2020 and 2021 Norway experienced comprehensive measures to prevent the spread of SARS-CoV-2, and in 2022 and 2023 Norway experienced a cost-of-living-crisis. It is expected that these events would negatively affect the population’s mental health. A Norwegian study found that despite the increasing trend, sick leave for common mental disorders were just as common in the control group as in the COVID-19 group between 2020 and 2022 [29]. Sick leave for mental disorders continued to increase in 2023 [13]. Another Norwegian study showed that people who tested positive for the Delta and Omicron variants of SARS-CoV-2 were no more likely to seek healthcare for anxiety/depression in the 126 days post-infection compared to those who tested negative [14]. In contrast, other international studies do show evidence of increased risk of depression after SARS-CoV-2 [3, 34].
Respiratory
R* (Respiratory) accounted for 14% of the total excess working person-days lost to medically certified sick leave in 2023, for an estimated economic loss of 2.3 billion NOK / 207 million USD.
R* (Respiratory) contained many individual ICPC-2 codes; R991 + R992 (COVID-19 suspected and confirmed) comprised 56% and 19% of all R* (Respiratory) working person-days lost to medically certified sick leave in 2022 and 2023 respectively (Table 3). In comparison, influenza comprised 4% and 10% of all R* (Respiratory) working person-days lost to medically certified sick leave in 2022 and 2023 respectively (Table 3).
This aligns with Norway’s strategy of maintaining a high level of SARS-CoV-2 infection [8,9,10].
Pain
Pain is a common post-acute sequela of COVID-19 [35], and the increase in 2023 from 2022 may be indicative of an increased morbidity in the general population due to the cumulative risk of post-acute sequelae, but other factors cannot be excluded.
Gastroenteritis
A small internal investigation was launched inside the Norwegian Institute of Public Health, but no similar reported increase was found in typical infectious disease pathogens that cause gastroenteritis (data/results not shown). A previous Norwegian study found that within people who had medically certified sick leave, those with R992 (Confirmed COVID-19) were more likely to have subsequent medically certified sick leave due to D73 (Gastroenteritis presumed infection) compared to those who did not have R992 [29]. Furthermore, gastrointestinal issues are well-known post-acute sequelae of COVID-19 [35]. These studies indicate that the increase may be associated with COVID-19, but other factors cannot be excluded.
Strep throat
Studies in people with post-acute sequelae of COVID-19 have observed immune dysregulation [35], which could make individuals more susceptible to post-COVID infections. One study in Israel found that patients infected with SARS-CoV-2 were at increased risk for streptococcal tonsillitis compared to those who tested negative [36]. The increase may be associated with COVID-19, but other factors cannot be excluded.
Hyperkinetic disorder
While there is no evidence for a link between COVID-19 and ADHD/ADD, there is strong evidence of neurological and psychological sequelae caused by COVID-19 [34, 35]. These sequelae, such as persistent memory problems [37] and cognition problems [38], may lead a patient to seek out their primary healthcare for an initial screening for ADHD/ADD or similar issues. That is, this increased trend may be partially explained by neurological and psychological post-COVID-19 sequelae causing individuals to seek healthcare for what they believe to be ADHD/ADD, but other factors cannot be excluded.
Deficits
The number of working person-days lost to medically certified sick leave due to some ICPC-2 codes was lower than expected (Table 2; Fig. 3). Generally, a decline in sick leave may be influenced by changes in political policy regarding sick leave and improved workplace/public health policies [39]. The deficit in medically certified sick leave for K76 (Ischaemic heart disease without angina) contrasts with Norwegian mortality statistics, where the age-standardized mortality rate of cardiovascular disease was higher than expected in both 2022 and 2023 [40, 41]. A plausible explanation may be that the excess mortality due to cardiovascular disease has reduced the number of people alive with cardiovascular disease, and hence the sick leave numbers have reduced. For less serious ailments such as N79 (Concussion) and L81 (Injury musculoskeletal NOS), the increase of remote work may have led to fewer people seeking medically certified sick leave.
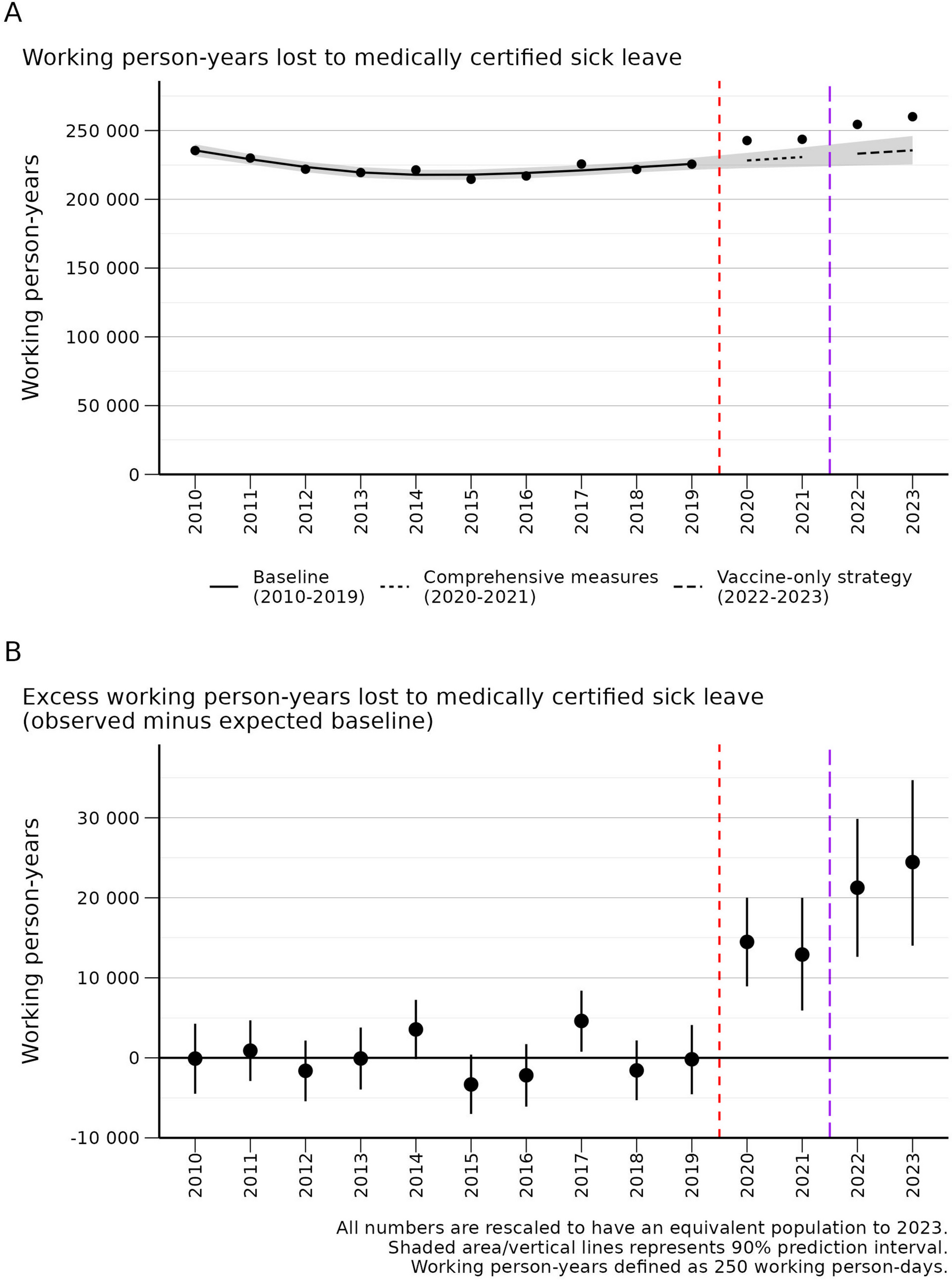
Excess working person-years lost to medically certified sick leave
In 2023, NAV paid out 583 billion NOK / 55 billion USD in benefits, of which 61 billion NOK / 5.7 billion USD corresponded to medically certified sick leave [42]. This study estimates an economic loss of 16.5 billion NOK / 1.5 billion USD in 2023 due to excess working person-years lost to medically certified sick leave.
The excess lost person-days of work in 2020–2021 may be partially explained by COVID-19 isolation rules [43]. The excess lost person-days of work increased from 2021 to 2022, as expected due to the cessation of comprehensive measures; a similar increase in health care utilization and inability to return to work or school was seen in the highly vaccinated West Australian population following the relaxation of infectious disease protective measures [44]. The excess lost person-days of work was higher in 2023 compared to 2022, which may be indicative of an increased morbidity in the general population due to the cumulative risk of post-acute sequelae [45]. High levels of absenteeism due to illness in 2023 have also been documented in Belgium [46], Germany [47], and the UK [48].
Lowered threshold for staying at home when ill
During 2020 and 2021, the public was advised to “stay at home when ill”. Because of this, it has been hypothesized that the excess sick leave in 2023 can be attributed to a lowered threshold for staying at home when ill. However, if this were the primary force driving the increase in medically certified sick leave, we would expect to see a flat increase across all diseases/symptoms. Instead, we see the opposite: A large increase in diseases/symptoms associated with acute and post-acute sequelae of COVID-19, and no increase or less of an increase in other diseases/symptoms.
Limitations
The fundamental limitation of this study is that it is a study based on aggregate data analyzing temporal changes. It is not possible to draw causal conclusions from this study, and there can be many reasons for the observed temporal changes, either in part or in whole.
Another limitation of this study is the lack of SARS-CoV-2 status at an individual-level. Due to a lack of testing for SARS-CoV-2 in Norway since early 2022, this was not possible to obtain.
A limitation of the NAV data is that it lacked information on age, which may have affected the results. To ascertain the importance of the age structure on the analyses, three analyses were rerun in NorSySS data, ignoring the age structure. The effect of ignoring age was minimal (ignoring of age structure vs. Table 2 results for thousands of estimated excess consultations in 2023): R** Respiratory infections (357 vs. 359), A04 Weakness/tiredness general (150 vs. 150), and D01 Abdominal pain/cramps general (77 vs. 76). It is likely that the analysis is robust to ignoring age because age is implicitly handled by the time trend.
A further limitation of this study is the inability to capture the full extent of COVID-19 spread due to the lack of reliable community transmission data. Nevertheless, our proxy measure based on vaccine efficacy and hospitalization rates provided valuable insights, showing positive temporal correlations with a range of health conditions.
An additional limitation of this study is that only 85 ICPC-2 code combinations were available from NorSySS, limiting the ability to compare with NAV data.
Strengths
The NAV data only contained medically certified sick leave. The number of days of self-certified sick leave allowed before a person transitions to medically certified sick leave varies by employer and collective bargaining agreement. Statistics Norway estimated that in the fourth quarter of 2023 83% of sick leave was medically certified and 17% self-certified. This study therefore has good coverage of sick leave data.
The primary strength of this paper is the breadth of the 556 ICPC-2 code combinations from the NAV data. In some cases (respiratory infections, fever, weakness/tiredness, strep throat), the NAV and NorSySS results agreed with each other, strengthening the findings. In addition, the high level of coverage in the NAV and NorSySS data provide a solid data backbone to the study.




留言 (0)