
記住我







This study was performed in a population-based prospective cohort study, the NEO study. All participants gave their written informed consent. The NEO study was approved by the Medical Ethics Committee of the Leiden University Medical Center (LUMC), Leiden, the Netherlands. The study design and population of the NEO study have been described previously [17]. Briefly, the NEO study was designed to investigate the mechanism that leads to obesity-related diseases. Men and women aged between 45 and 65 years at baseline (September 2008 to September 2012) with a self-reported body mass index (BMI) of 27 kg/m2 or higher living in the greater part of Leiden were invited to participate in the NEO study. In addition, all inhabitants aged between 45 and 65 years from one municipality (Leiderdorp) were invited, irrespective of their BMI. Participants were invited for a baseline visit at the NEO study center of the LUMC after an overnight fast. Before the baseline visit, participants completed questionnaires at home to report demographic, lifestyle, and clinical information. At baseline visit, all participants underwent an extensive physical examination including anthropometry and blood sampling. Research nurses recorded names and dosages of current medication used in the month preceding the study visit. After the baseline visit, participants were followed for the occurrence of type 2 diabetes.
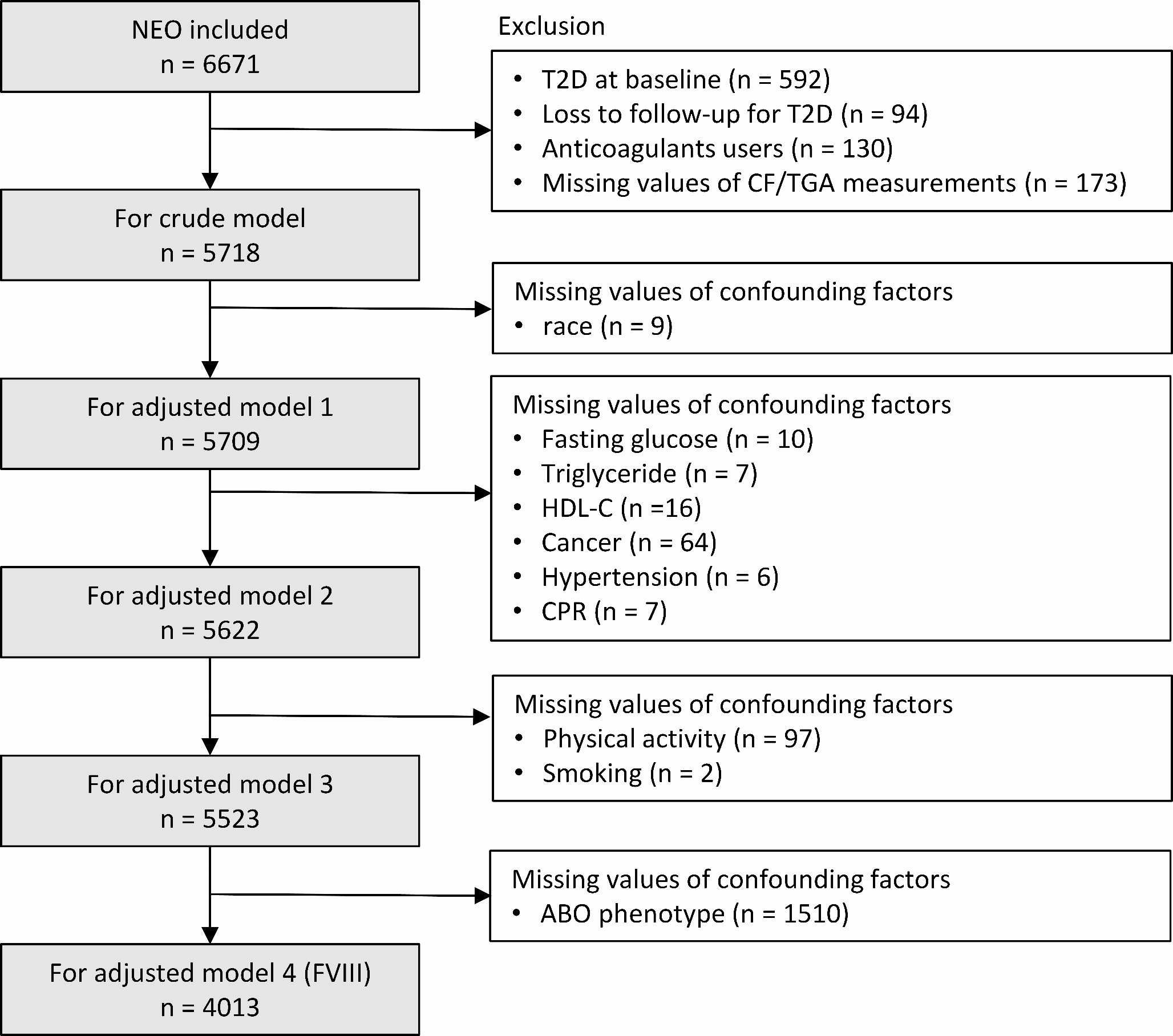
Participants who had been diagnosed with type 2 diabetes before or at the baseline visit (n = 592), or those without any follow-up information regarding the incidence of type 2 diabetes (n = 94) were excluded for the present study. We also excluded participants who used vitamin K antagonists or heparin at the baseline visit (n = 131) as these medications may influence coagulation factor levels and thrombin generation potential. As direct oral anticoagulants (DOACs) were not commonly used in the Netherlands during the NEO baseline recruitment, the NEO study did not collect information for the use of DOACs. We additionally excluded participants with missing data on any of the exposures, the mediator, and confounders (n = 444). In the analyses involving ABO blood group, participants with missing data for ABO blood group were additionally excluded (n = 1510). Figure 1 shows the selection of participants for the present study.
Fig. 1
Flow chart of participants inclusion in the present study
Abbreviations: NEO: the Netherlands Epidemiology of Obesity study; FVIII: coagulation factor VIII
Data collectionHemostatic factors and thrombin generation parametersCoagulation factor levels and parameters of thrombin generation potential were measured from fasting blood samples collected at the baseline visit. Fasting blood samples were drawn into tubes containing 0.106 M trisodium citrate (Sarstedt, Etten-Leur, the Netherlands). FVIII, FIX, and FXI activity were measured using a factor-specific clotting assay with ACL TOP 700 analyzer (Werfen, Barcelona, Spain). Fibrinogen levels were measured by the method of Clauss [18]. A thrombin generation assay was performed using the Calibrated Automated Thrombogram® (Diagnostica Stago, Asinères, France) following the instructions of the manufacturer [19]. In brief, platelet-poor plasma samples were added to the assay reagent including phospholipids and a very low tissue factor concentration (86194,TS31.00, STAGO, France). A Fluoroskan Ascent fluorometer (Thermo Scientific, Waltham, MA, USA) detected the fluorescent signal to represent thrombin generation. Five thrombin generation parameters were estimated using the Thrombinoscope software (Thrombinoscope BV, Maastricht, the Netherlands). Lag time measured in minutes indicates the time from induction to the initial thrombin generation. Endogenous thrombin potential (ETP) corresponds to a measure of the total amount of thrombin generation, corresponding to the area under the curve of thrombin generation curve. Peak height measured in nM represents the highest point of thrombin level. Time-to-peak measured in minutes corresponds to the time from the induction to the peak. Velocity indicates how fast thrombin levels rise from the initial point of thrombin generation to the peak height.
Incidence of type 2 diabetesNew diagnoses of type 2 diabetes were extracted between October 2017 and July 2018 from the electronic health records of the general practitioners (GP) of the participants. Data from the first extraction (July 2012- November 2013) were added to this extraction [20]. Details of the extraction process are provided in the Online supplemental method. Briefly, health records were screened for the International Classification of Primary Care (ICPC) code T90 (diabetes mellitus) or T90.02 (diabetes mellitus type 2) and the prescription of specific medication corresponding to the Anatomical Therapeutic Chemical code A10 (drugs used in diabetes). The medication list of participants was also checked for the use of insulin, metformin, and sulfonylurea derivatives (including search terms for brand names and abbreviations). The index date was defined by the first date of an ICPC-coded diagnosis, or the first date of prescription of anti-diabetic medication. In case of uncertainty, we checked for a preceding diagnosis of disturbed glucose tolerance (ICPC code A91.5), high glucose concentration data in any lab record (if available) and we read the free text in the health records for signs of diabetes. These findings were discussed by the NEO study adjudication committee to decide on a diagnosis. If the diagnosis remained uncertain, the GP of the participants was contacted to confirm the date and diagnosis. Time of follow-up was defined as the number of days between the baseline visit and the date of diagnosis, or censoring due to death, loss to follow-up, or the end of the follow-up (extraction date at the GP in 2013 or 2018), whichever came first. For participants without medical records from their GP more than a year between the last contact and data extraction, we additionally defined a minimized follow-up time for sensitivity analyses as the time between the baseline visit and the date of the last contact with GP because it was unknown whether the participants did not visit their GP afterwards or had switched to another GP.
CovariatesOn the baseline questionnaire, participants reported age, sex, and family and personal medical history. We considered active cancer patients as those who have been diagnosed within 5 years before baseline and have not been medically cured based on self-report. Hypertension was defined as a systolic blood pressure > = 140mmHg or diastolic blood pressure > = 90mmHg or using antihypertensive drugs. Self-identified race was reported in eight categories, which were grouped into white and others. Participants reported the frequency and duration of their physical activity during leisure time over the past 4 weeks on the Short Questionnaire to Assess Health-enhancing activity, which we expressed in MET-hours per week. Tobacco smoking was reported in three categories with current smoker, former smoker, and never smoker. In women, we grouped the use of contraceptives and hormone replacement therapy into current and past or never users. Menopausal status was classified as premenopausal and perimenopausal or postmenopausal, according to information on oophorectomy, hysterectomy, and self-reported state of menopause in the questionnaire. BMI was calculated by dividing the weight in kilograms by the height in meters squared measured during physical examination. Fasting serum glucose and triglyceride concentrations were measured with enzymatic calorimetric assays (Roche Modular P800 Analyzer, Roche Diagnostics, Mannheim, Germany) and fasting serum high-density lipoprotein cholesterol (HDL-C) concentrations with third-generation homogenous HDL‐C methods (Roche Modular P800 Analyzer, Roche Diagnostics, Mannheim, Germany). ABO blood group was determined by the four ABO genetic variants (rs8176719:insC, rs7853989:G > C, rs8176749:G > A, rs8176750:delC) using the imputed genotype data in the NEO study, which has been described in details before [21]. The serum concentrations of C-reactive protein (CRP) were determined using a high-sensitivity CRP assay (TINA-Quant CRP HS system and Modular P800; Roche) [22]. Glycoprotein acetyl (GlycA) concentrations, as the potential mediator, were measured in plasma samples using the Nightingale high throughput NMR metabolomics platform [23].
Statistical analysisBaseline characteristics of the study population are presented as absolute numbers and percentages for categorical variables, and continuous variables as medians with interquartile range (IQR) or means with standard deviation (SD). The cumulative incidence of type 2 diabetes was calculated taking the competing risk of death into account. Incidence rates of type 2 diabetes per 1000 person-years with 95% confidence intervals (CI) were calculated for quartiles of coagulation factor levels and thrombin generation parameters. We used Cox proportional hazards regression to calculate hazard ratios (HR) and 95% CI as estimates of the association between the levels of coagulation factor and thrombin generation parameters and the incidence of type 2 diabetes. We adjusted the crude model for age, sex, and race in model 1. In model 2, BMI, baseline levels of fasting glucose, triglyceride, CRP, HDL-C, active cancer, and hypertension were further added, which were expected to have confounding effects. In model 3, we added physical activity, smoking, menopausal status, oral contraceptive use, and hormone replacement which likely have confounding effects. Specifically for the association between FVIII levels and type 2 diabetes, ABO blood group was added to the model 3. In model 4, we added GlycA to examine the mediation effect on the association between coagulation factor levels as well as thrombin generation parameters and the incidence of type 2 diabetes. The proportion of mediation was estimated via R package “CMAverse” with bootstrap 95% CI and p-values [24]. The proportional hazards assumption was checked by the Schoenfeld residuals test (Supplemental Figs. 1–5). For models in which the proportional hazard assumption was violated, we added an interaction term between time categorized in periods of 0.5 years and the variable for which the proportional hazard assumption was not met to the model. All analyses were performed using the coagulation factors and thrombin generation parameters as continuous exposure and repeated after categorizing exposures in four groups using their quartiles, using the first quartile as the reference except for lag time and time-to-peak for which we used the fourth quartile as the reference.
In addition, stratified analyses, and sensitivity analyses were performed. First, we stratified all analyses by sex. Second, we aimed to stratify all analyses by BMI of 27 kg/m2 (the cut-off value for overweight in the original NEO study). Due to the limited number of participants with BMI less than 27 kg/m2, analyses were performed only participants with BMI of 27 kg/m2 or higher. In addition, we also performed several sensitivity analyses. First, the follow-up was restricted to the date of the last contact with GP for participants who lacked information in their medical records for more than a year between the last contact and data extraction. Second, we performed a landmark analysis to avoid reverse causation by including only participants who were still in the study after one year. Third, as GlycA is a marker of systemic inflammation, we excluded participants (n = 72) with self-reported autoimmune diseases at baseline (i.e., systemic lupus erythematosus, rheumatoid arthritis, and psoriatic arthritis). Lastly, we calculated E-values based on the effect estimates and confidence intervals to investigate the potential impact of unmeasured confounding [25]. All statistical analyses were performed using R version 4.3.0.
Data and resource availabilityThe data that support the findings of this study are not openly available due to the privacy of the participants of the NEO study and legal reasons (NEO study participants did not sign informed consent to make their data publicly available). The data will be made available upon request to interested qualified researchers. Data requests should be sent to the NEO Executive Board, which can be contacted via https://www.lumc.nl/org/neo-studie/contact/. Scripts for the analysis are available upon request to the authors.
留言 (0)