
記住我



The spectrum of fibrotic interstitial lung diseases (ILD) shares pathogenetic mechanisms of inflammation and fibrosis not only involving the interstitial space, but also the alveolar epithelium and the vascular endothelium [1, 2]. While light microscopy only allows for a limited perception of such processes [3, 4], transmission electron microscopy (TEM) enables deeper insights into cellular and subcellular structures, and can potentially visualize earlier disease-specific alterations [5]. Transbronchial lung cryobiopsy (TBLC) has proven a reasonable balance between quantity and quality of retrieved tissue and procedural risk, with a diagnostic yield similar to surgical lung biopsy [6]. As TBLC samples from fibrotic ILD patients have not been systematically studied by TEM so far, we assessed the feasibility of this approach and particularly microvascular alterations in a cohort of consecutive fibrotic ILD patients undergoing routine bronchoscopic evaluation at Kepler University Hospital Linz, Austria in the year 2023.
Patients with fibrotic ILD (i.e. with computed tomography evidence of a reticular pattern, traction bronchiectasis or honeycombing) provided written-informed consent to additional TEM evaluation 1 to 2 TBLC samples, given there was sufficient biopsy material for routine pathology examination. TBLC was performed according to current state-of-the-art [6], under general intravenous anaesthesia with rigid bronchoscopic intubation and jet ventilation. A balloon catheter for bleeding control was placed and a minimum of 4 TBLC samples were retrieved from two different lung segments under fluoroscopic control. Samples for TEM were fixed in a cacodylate-buffered solution of 2.5% glutaraldehyde and 2% paraformaldehyde, postfixed in 1% osmium tetroxide, and embedded in epoxy resin. Ultrathin sections were analyzed in a Zeiss LEO EM 910. Biopsy samples intended for routine light microscopy were fixed in 4% formalin and stained with Hematoxylin-Eosin (HE). For controls, subpleural fresh lobectomy tissue from lung cancer patients unaffected by ILD, participating in another study was sampled both by a cryoprobe inserted through a pleural incision, and by excision without freezing.
Of 18 patients enrolled, one sample for TEM analysis did not contain sufficient alveolar lung tissue, and in one patient, endobronchial bleeding kept the investigator from acquiring an additional sample for TEM. In the remaining 16 patients, TEM revealed good ultrastructural preservation and enabled the definition of a standardizable set of cryoartifacts as compared to three non-frozen controls: The cryosampled tissue was predominantly characterized by expanded interstitial spaces and a reduced electron density of cytoplasmic areas. This was commonly accompanied by an inflation of membranous compartments such as endoplasmatic reticula, and by mitochondrial swelling together with a loss of inner membrane structure and coherence. (Fig. 1a-c).
Fig. 1
Representative images of alveolar capillaries and surrounding tissue in an unfrozen control (a), a control frozen to a cryoprobe (b), and a cryobiopsy sample of an ILD case (c). In cryobiopsy specimens, mitochondria (arrows) are dilated and lack inner membrane structure, the endoplasmatic reticulum (white arrowheads) and other membranous compartments appear bloated. Some interstitial spaces are dilated (asterisks). bl: basal lamina, cf.: collagen fibrils, ef: elastic fibers, E: endothelial cell, Er: erythrocyte, F: fibroblast, P1: type 1 pneumocyte, arrows: mitochondria, white arrowheads: endoplasmic reticulum, asterisk: dilated spaces. Scale bars: 1 μm
Fig. 2
Representative images of alveolar capillaries and surrounding tissue showing different grades of TEM endothelial alterations. In grade 1 samples (a, b) capillary endothelial cells show a normal, flattened morphology, in grade 2 (c, d) they are partly thickened and form luminal pseudopodial protrusions (black arrowheads). This is further increased in number and size in grade 3 (e, f), up to complete vessel obturation (f). bl: basal lamina, cf.: collagen fibrils, ef: elastic fibers, E: endothelial cell, Er: erythrocyte, F: fibroblast, P1: type 1 pneumocyte, black arrowheads: endothelial protrusions. Scale bars: 1 μm
As compared to controls, the alveolar parenchyma of ILD lungs was characterized by larger deposits of collagen, elastic fibres, and presence of fibroblasts (Fig. 2c-f). In several cases, the basal membrane layers between capillary endothelia and pneumocytes were thickened, interspersed with collagen fibres and fibroblast protrusions (Figs. 1c and 2d).
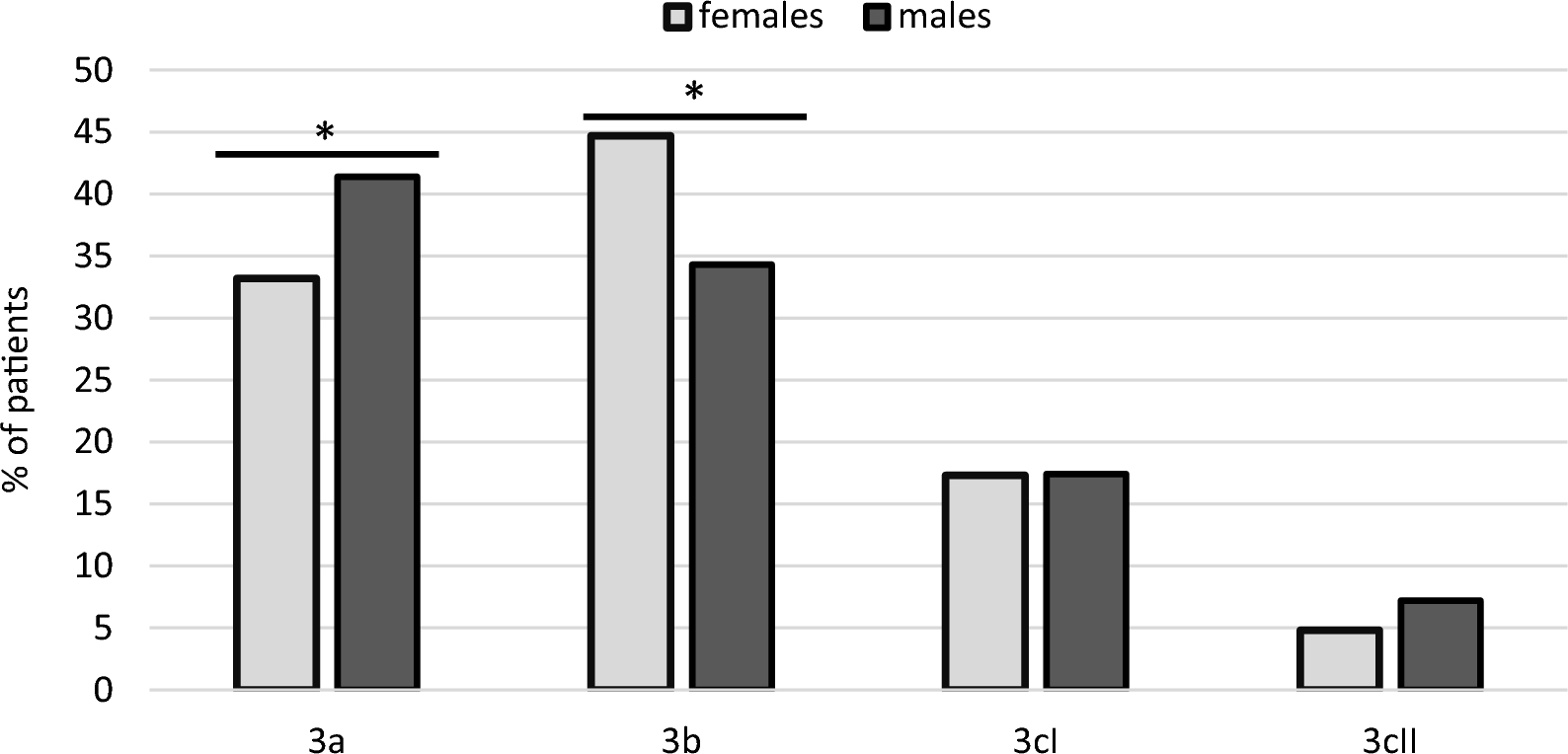
The most evident TEM findings concerning microvascular morphology in a considerable fraction of patients were a marked transformation of capillary endothelia towards a thickened cell shape as compared to their normal squamous appearance, and the presence of numerous pseudopodia protruding into the lumina. Endothelial thickenings, either cushion-like or along the entire perimeter, together with the pseudopodia even lead to a complete capillary obstruction in extreme cases (Fig. 2c-f). These endothelial abnormalities were staged as grade 3 (highly present) in 4 patients (25%), as grade 2 (moderately present) in 7 patients (43.8%), and as grade 1 (largely absent) in 5 patients (31.3%). (Fig. 2)
Although less distinct than in TEM, routine light microscopy also revealed pathological vascular features in several patients, including swelling and increased number of endothelial cells and focal vessel proliferation. Analogously graded by severity, these were correlated with endothelial alterations detected in TEM (Table 1).
Table 1 Baseline patient characteristics, laboratory, lung function and light microscopy results of all patients, and according to grades of TEM endothelial alterationsAs shown in Table 1, patients with more advanced endothelial alterations were younger, more hypoxemic and had lower lung volumes and diffusion capacity. Radiologically, they more frequently exhibited a non-specific interstitial pneumonia (NSIP) pattern, had a higher lymphocyte count in broncho-alveolar lavage (BAL), and more frequently fulfilled the serological domain of interstitial pneumonia with autoimmune features. However, the grade 3 patients did not exhibit other classical signs of acute inflammation, neither locally such as lymphocyte aggregates and presence of lymph follicles in light microscopy, nor systemically such as elevations in relevant blood biomarkers like CRP and LDH (Table 1).
Our results demonstrate that diagnostic TEM examination of TBLC samples from ILD patients is feasible and enables high-quality ultrastructural imaging, with cryoartifacts occurring in a standardized fashion. Primarily, this implies that our described approach can be considered as a method for future research of fibrotic ILD, especially concerning microvascular processes. The number of patients in our study was low, so that no definite conclusions on the origin and significance of the vascular alterations detected can be drawn. Still, our findings of marked endothelial abnormalities in a subgroup of ILD patients once more emphasize the prominent role of the pulmonary endothelium in the pathophysiological processes underlying fibrotic ILD [2].
Although patients with stage 3 TEM endothelial alterations had a higher BAL lymphocyte count, presence of autoantibodies, and a radiological NSIP pattern in most cases, they exhibited rather less pronounced light microscopy signs of inflammation and inconspicuous levels of relevant systemic inflammation biomarkers. Such discrepancy between advanced endothelial transformation and the absence of fully developed local inflammation may indirectly correlate with the results of a post-mortem study on fatal COVID-19 pneumonia, where TEM failed to reveal significant endothelial abnormalities despite evidence of severe alveolar epithelial damage [7].
Of interest, similar luminal endothelial pseudopodia formation as seen in our cohort has been reported as a response to lack of capillary fluid flow in rat skeletal muscles [8], thus the observed capillary alterations could represent a response to altered blood flow conditions and shear stress in lung areas affected by ILD.
Research on systemic sclerosis and pulmonary arterial hypertension implies that microvascular remodelling could also be indicative of endothelial to mesenchymal transition [9, 10]. Alternatively, as the TEM stage 3 patients in the present study had lower spirometry, diffusion capacity and oxygenation biomarkers, the observed endothelial alterations could indicate hypoxemia-induced angiogenesis, however the entirely endoluminal fashion of the observed processes does not appear typical of new vessel formation [2].
The limitations of our reported analyses include the small sample size and the lack of the possibility of comparison with other, similar studies and with healthy individuals. The small control group was derived from cancer patients and the tissue from which the control biopsies were taken had been ischaemic for up to one hour before sampling, while cryobiopsies from ILD cases were processed immediately, within seconds after thawing. Also, given the advanced age of the patient population, it cannot be precluded that processes associated with normal ageing or with pulmonary comorbidities may have contributed to the observed endothelial alterations. Alveolar capillaries arise both from the systemic as well as from the pulmonary circulation and it cannot be clarified with certainty, whether the observed alterations are specific to either system. Also, not only the heterogeneity of ILD entities present in the studied cohort, but also the possible spatial heterogeneity of interstitial changes within a single patient’s lung could impair the comparison between cryobiopsy samples analyzed by TEM and those undergoing usual microscopic evaluation.
We suggest that TEM evaluation of TBLC samples from ILD patients is feasible, could enable novel insights into ILD pathophysiology, and should therefore be evaluated further in basic and clinical research. The observed microvascular alterations warrant evaluation in larger cohorts with a refined methodology.
留言 (0)