Hypertensive emergencies represent a form of acute severe hypertension with multiple organ damage and should bring about poor prognosis unless appropriately treated. Cardiac, renal and retinal disease are the commonly observed complications and traditionally, an acute and marked elevation in BP is recognized to be responsible for the development of these organ injuries. There is proposed, however, an additional thesis that enhanced RAS activity may play a substantial role in the pathogenesis of the acute organ injuries in hypertensive emergencies [3, 4, 14]. We therefore attempted to characterize the clinical features underlying the acute hypertensive organ damage, based on the levels of BP and RAS, especially aldosterone.
Role of aldosterone in hypertensive emergency-associated organ damage
Evidence has been accumulated that RAS constitutes a pivotal aspect in the pathological process of malignant hypertension, a major subset of hypertensive emergencies. Thus, aldosterone, acting as a hormonal mediator, contributes to the development of retinopathy through vascular endothelial dysfunction and retinal inflammation [5, 15,16,17,18]. In the present study, we found that the patients with severe retinopathy had higher aldosterone levels along with systolic and diastolic BP (Fig. 2, Supplementary Fig. 1). Although acute severe hypertension-induced organ damage is recognized as the consequence of the organ ischemia and/or the hyperperfusion-induced capillary leakage attributed to disrupted blood flow autoregulation [19], elevated aldosterone levels may also act in concert with the hemodynamic factor to cause severe retinopathy [5]. Furthermore, aldosterone could promote hypertrophic changes in cardiomyocytes [20] and may contribute to the development of concentric LVH [6].
In addition to the classic action on renal electrolyte and body fluid balance, excess aldosterone may exert deleterious effects on various organs [5,6,7]. The present study revealed that higher plasma aldosterone was associated with severe renal impairment (eGFR < 30 mL/min/1.73 m2) and the development of TMA (Fig. 2 and Supplementary Fig. 1). Because aldosterone causes endothelial dysfunction [15, 16], acute complications of TMA and renal impairment may be relevant to the previous reports showing aldosterone-mediated endothelial injury independent of renin or angiotensin [17, 18]. Elevated aldosterone may therefore facilitate multiple organ injuries under the milieu of acute severe hypertension.
Of note, the present study showed that both renal impairment and TMA were closely associated with elevated aldosterone, but neither systolic nor diastolic BP differed between the presence and the absence of these complications (Fig. 2A and D and Supplementary Fig. 1). Akimoto et al. [7] found higher aldosterone levels in patients with TMA than in those without TMA. An experimental study also revealed that aldosterone played a crucial role in the pathogenesis of TMA, independently of hypertension, in stroke-prone spontaneously hypertensive rats [20]. Interestingly, van den Born et al. [10] demonstrated a close relationship between TMA and renal dysfunction in patients with malignant hypertension. They also showed that RAS activation was associated with enhanced microangiopathic damage and renal dysfunction [3]. It is reasonably inferred therefore that aldosterone could participate in the development of microangiopathy and accelerate the progression of renal impairment.
We observed 10 cases with HFrEF (i.e., EF < 40%). Although chronic exposure to excess aldosterone was associated with collagen accumulation in the myocardium [21], we failed to show any significant difference in plasma aldosterone concentration between the subgroup with EF < 40% and that with EF ≥ 40% (Fig. 2E). Similarly, the patients with cerebral infarction also manifested no differences in these three parameters (Fig. 2F) but higher LDL-cholesterol levels. Other factors such as hypertension history, the presence of diabetes and the level of renal function may need to be taken into consideration.
Number of complications and BP/aldosterone
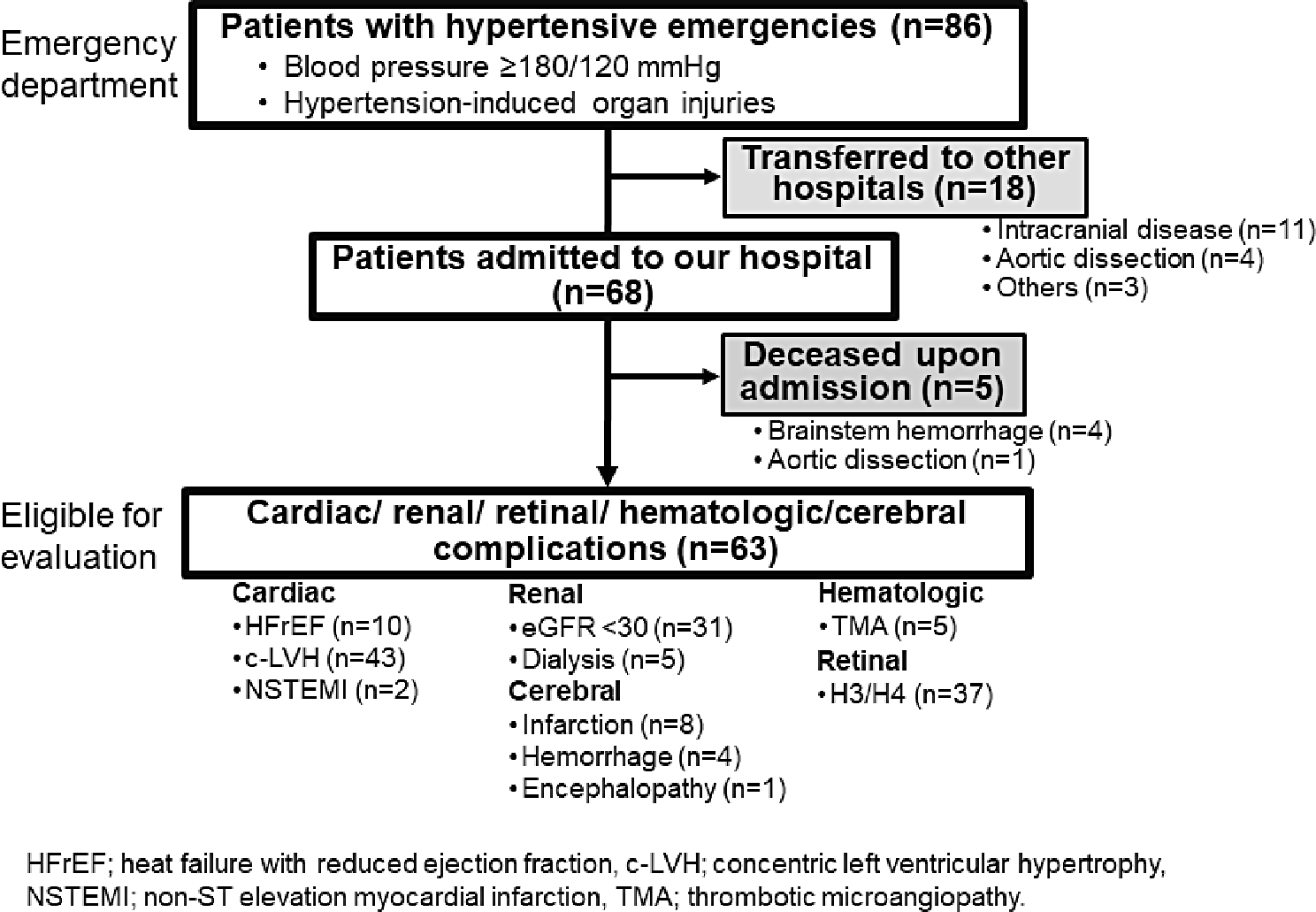
The present study demonstrated that the incidence of each complication varied depending on the target organs (i.e., 49.2%, 80.4%, 72.9%, 7.9%, 16.9%, 12.7%, and 6.3%, for kidney impairment, severe retinopathy, concentric LVH, TMA, HFrEF, cerebral infarction, and cerebral hemorrhage, respectively, p < 0.001, Fig. 2). Whereas we arbitrarily defined some of these complications, the differences in the incidence of the complications could be attributed to the diverse vulnerability of the organs to BP and aldosterone. Of note, the present study failed to include the 4 patients with brainstem hemorrhage because they died before detailed evaluation (Fig. 1). When these patients were incorporated in the overall incidence calculation, 25% of the 68 patients admitted to our hospital with hypertensive emergencies had cerebrovascular disease. Furthermore, this rate could have been higher if all patients had undergone detailed brain imaging.
In our study, 44 patients (i.e., 69.8%) had multiple organ injuries at the time of admission, and as many as 27 cases (i.e., 42.9%) possessed 3 or more complications (Fig. 3A). Among these, 22 cases manifested a triad of acute kidney impairment, severe retinopathy and concentric LVH (i.e., a∩b∩c, Fig. 3B) and had a higher aldosterone concentration (321 [IQR: 218–553] pg/mL, Supplementary Table 1). These observations lend support to the premise that aldosterone is involved in the pathophysiology of the multiple organ injuries in hypertensive emergencies. Indeed, a strong correlation was noted between the number of complications and plasma aldosterone levels (Rs = 0.50, p < 0.001, Fig. 4B). The fact that higher plasma aldosterone (≥ 250 pg/mL) is associated with 3 or more complications also indicates a close relationship between these two factors (Fig. 4C).
The incidence of each organ injury may vary depending on the multiplicity of the complications in hypertensive emergencies. Thus, the incidence rates of severe kidney impairment, concentric LVH and retinopathy rose in parallel with the number of the complications (Fig. 5). Additionally, concentric LVH and retinopathy were found more frequently than other organ injuries among the patients with 1 or 2 complications in whom plasma aldosterone levels were not elevated. In contrast, TMA was observed exclusively in patients with 4 complications. Finally, no apparent association was seen between the number of complications and the incidence of cerebral infarction or hemorrhage. These findings thus suggest that the organ damage in hypertensive emergencies is mediated by at least two mechanisms, including a hemodynamic burden and a hormonal factor to which each organ has variable susceptibility. Alternatively, antecedent treatment of hypertension and pre-existing metabolic factors may modify the severity of organ damage at presentation [22] although our study shows a modest impact of smoking habit on concentric LVH (Supplementary Table 2).
Intriguingly, all cases with TMA were found among the subgroup with a triad of impaired renal function, severe retinopathy and concentric LVH (Fig. 3B) and hence had 4 complications. This subgroup could therefore be regarded as manifesting a severer form of hypertensive emergencies. Although aldosterone plays a pivotal role in the development of TMA (Fig. 2D and Supplementary Fig. 1) [7, 20], there was found no difference in its concentration between the subgroup with TMA and that without TMA when evaluated among the population with the triad (Supplementary Table 1). Since endothelial injury constitutes a major determinant of TMA, additional factors favoring endothelial damage may predispose this population to TMA under the high aldosterone milieu; smoking-related vascular injury could be a possible factor (Supplementary Table 1) [23, 24].
Limitation
The results from our cross-sectional study contain several caveats to be mentioned. This study was conducted in a single medical center located in the suburbs of Tokyo and the patients enrolled in this study might have some bias that affected patient profiles. Indeed, 79.4% of the patients were aware of hypertension but only 22.0% had been receiving medical management (Table 1) and many of the remaining subpopulation discontinued the treatment, i.e., non-adherence to antihypertensive medications [1]. Furthermore, quite a few patients did not consult a doctor with unclarified reasons. The rate of smoking habits (54.0%) was also higher than that in the general population in Japan (16.7%, https://www.health-net.or.jp/tobacco/statistics/kokumin_kenkou_eiyou_report.html) though smoking is associated with the development of malignant hypertension [25]. It requires more thorough evaluation to clarify whether the diverse patient profiles or event rates affected our observations.
Both absolute BP levels and the rate of the change in BP determine acute hypertension-induced organ damage [1]. In this study, however, many of the patients were non-adherent to medications or saw a doctor at variable intervals, making it difficult to assess systematically the pace of changes in BP before admission. More sophisticatedly designed studies will clarify the role of the pace of rise in BP and/or aldosterone in the development of acute hypertension-induced organ damage.
Finally. the present study evaluated the role of aldosterone as a representative of RAS in hypertensive emergencies. Although angiotensin II constitutes one of the most potent factors determining the development or aggravation of malignant hypertension, its measurement is not readily available in clinical practice, compared with PRA or aldosterone. In this regard, we also measured PRA (Supplementary Table 3, Supplementary Fig. 3) and found that both aldosterone and PRA levels changed in a similar manner in hypertensive emergencies, thus confirming the credibility of aldosterone in the assessment of RAS activity.



留言 (0)