We provided results from apixaban drug level monitoring in hemodialysis patients on different dosing regimens. We investigated risk factors for increased drug level, an analysis with regard to bleeding events and provided a literature comparison to non-CKD populations.
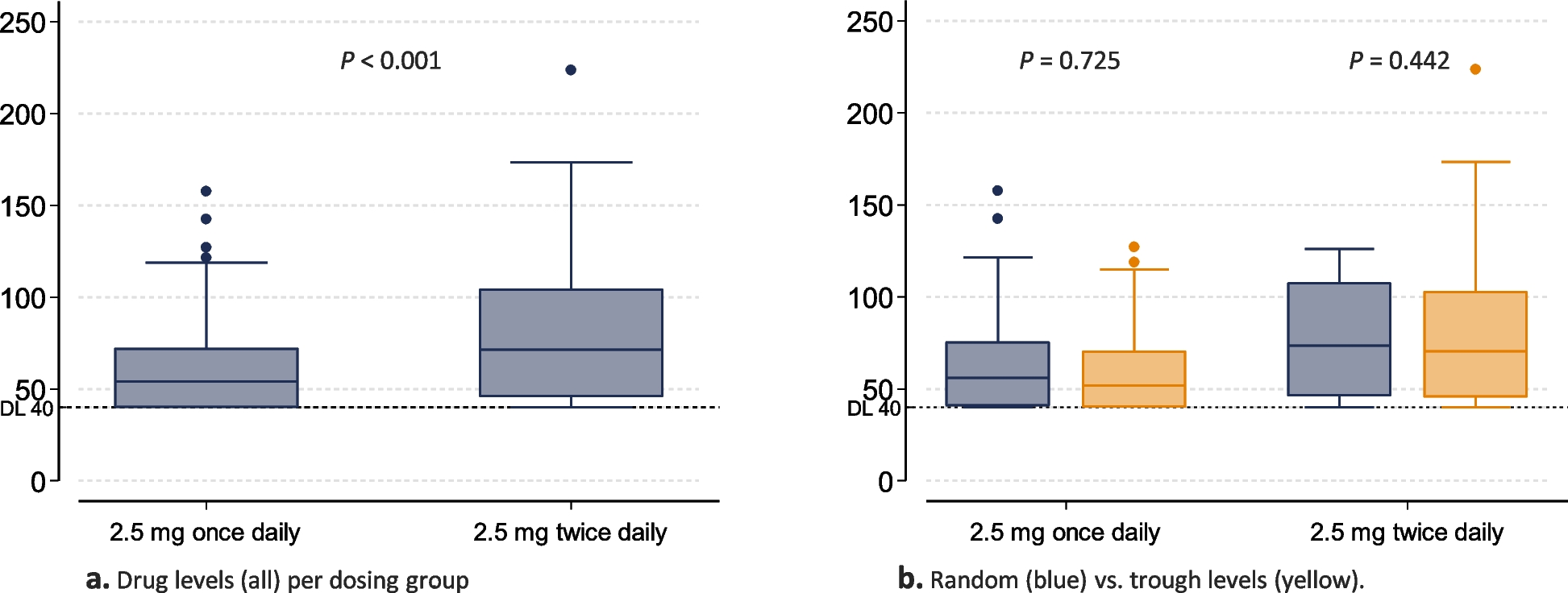
With regard to a 2.5 mg twice daily dosing in patients on hemodialysis, our median drug levels were comparable to those from non-CKD-populations, taking the same reduced dose [30,31,32], published among others by the European Union summary of product characteristics [2]) although with a larger 5th – 95th percentile range (71 [< 40 – 141] versus 56 [24 – 103], 79 [34 – 162], 63 [11 – 90] ng/mL). However, our median (5th – 95th percentiles) drug levels appeared considerably lower in comparison to non-CKD-reference populations taking the standard dose of 5 mg twice-daily [30,31,32]. Hence, looking at drug level data only, our results suggest, that 2.5 mg twice daily is not associated with overtly increased drug exposition compared to non-CKD patients for whom licensure studies were performed. On the contrary, our results rather suggest, that with 2.5 mg twice daily (14 % below detection limit), and even more so with 2.5 mg once daily dosing (30 % below detection limit), individual patients are probably under-dosed, arguing for more routine drug monitoring. It is worth mentioning however, that some patients on 2.5 mg once daily dosing showed comparable drug level to other patients on 2.5 mg twice-daily schedules. In addition, 2.5mg once daily dosing might still confer valuable prophylactic benefits e.g. for long-term patency of venous accesses.
Our analysis did not include a patient on a 5 mg twice-daily dosing schedule. Pokorney et al. found AUC0-12 values of patients on hemodialysis with 5 mg twice daily significantly higher compared to non-CKD participants from the ARISTOTLE trial (2475 ng/mL×h versus 1374 ng/mL×h) taking the same standard dose [19]. Interestingly, values in patients on hemodialysis were comparable to ARISTOTLE participants with an eGFR of 15 - 59 ml/min/1.73m2. These results again argue for contributory drug monitoring.
It needs to be emphasized, that target ranges for apixaban drug levels are not established and that existing literature does not support valid assessment of efficacy or bleeding risk via drug monitoring [19, 33, 34]. However, risk-benefit analysis regarding anticoagulation in hemodialysis is challenging and recommendations regarding apixaban are contradictory. Thus, drug level monitoring does provide clinicians with valuable information for improved individual decision making, especially if drug levels are at the edges of the spectrum (e.g. below detection limit or beyond the 95th percentile of non-CKD reference populations). Here, our study provides valuable practical guidance to improve patient safety.
Trough levels did not differ from random levels. An important factor here is the retrospective nature of the study with substantial inaccuracies regarding the time point of drug intake. E.g. if the treating team forgot to inform the patient to wait with the apixaban intake until trough level measurement had taken place, or if the patient did not comply with the agreed schedules, measurements labeled as trough could provide levels shortly after or even days after the last intake. These inaccuracies have to be considered for the interpretation of all drug levels. In cases of overtly low or overtly high drug levels, missing intakes or accidental peak level ascertainments should be ruled out. Furthermore, there is considerable intra- and inter-individual variability of drug levels, a well-known challenge of apixaban drug level monitoring [6, 33]. However, even under the real-live conditions of our investigation, no exacerbation of drug levels was seen.
None of the dialysis-associated parameter were independently associated with drug levels. This was somewhat unexpected. Apixaban has a molecule size of 459.5 Dalton, a protein binding of 87 % and a distributional volume of 21 L [1]. Thus, a fractional removal by hemodialysis is expected. Small prospective pharmacokinetic studies show a reduction in AUC by hemodialysis of -14 % (pre/post) [8] and -26 % (AUC-48h) [9] for a 5 mg dose and a AUC-48h reduction of -48 % for a 2.5 mg dose [9]. Potentially, our inter-individual differences in dialysis dose were too small. However, in light of low sample numbers and retrospective analyses, interpretation of multivariable regression results is limited. Intake of a second dose of 2.5 mg of apixaban per day was consistently associated with higher drug level. This highlights at least a rough relationship between amount of intake and steady state drug level, again supporting drug monitoring as an additional mean for individual dose finding.
Our analysis does not suggest drug accumulation over time independent of dosing regimen and length of follow-up. In contrast, pharmacokinetic analyses revealed significant accumulation in hemodialysis patients during the first 8 days [23]. Our data did not allow valid analyses of drug levels within the first few days after starting the drug. However, with regard to our follow-up period (IQR 5.5 - 21 months), our data clearly support the picture of a non-accumulating steady state.
Our study has several strengths. It is the second largest analysis of apixaban drug levels in hemodialysis to date with the longest follow-up. It is the only investigation incorporating apixaban drug levels from 2.5 mg once daily dosing and comprehensive dialysis-related covariates. In addition, we provide a comparative review to drug levels from non-CKD populations facilitating interpretation of drug levels and supporting sensible decision making regarding appropriate dosing.
The main limitations of our study are its retrospective nature, limiting precise specification of timing of drug intake and a reliable integration of residual kidney function. Drug levels of our study however, do picture long-term results from a tertiary care real-life setting. The analysis of bleedings must be considered exploratory as drug level measurements were infrequent and number of patients and bleeding events were small. The selection of covariates is overly inclusive. However, selected dialysis-associated factors represent important confounders, which have not been comprehensively investigated in studies of apixaban in patients on hemodialysis.



留言 (0)