
記住我






Pain scores were available for 61 participants who provided 361 reviews, including 25 individuals with RDEB-S (175 reviews), 22 with RDEB-I (108 reviews), 9 with RDEB-Inv (56 reviews), 4 with RDEB-Pru (17 reviews), and 1 with RDEB-PT (5 reviews). Table 1 shows participant demographics at index review.
Disease severity scores (iscorEB, BEBS) at index review were higher for participants with RDEB-S and RDEB-Pru than those with intermediate and inversa subtypes (Table 2). Similarly, severe and pruriginosa participants had higher QOLEB scores (indicating greater negative impact on QOL) and spent more time on dressing changes than the other subtypes (Table 2). Similar findings were revealed on consideration of all 361 reviews (Supplementary Table 1).
Table 1 Participant characteristics by RDEB subtype (n = 61)Table 2 RDEB severity at index review (n = 61)Intensity of background and procedural painMost participants (93%) reported pain at index review (Table 3), including all those with RDEB-S and RDEB-Pru. Fifty individuals (80%) reported both background and procedural pain. Only three participants with RDEB-I (2 adults, 1 child) reported no background pain at all reviews (n = 13). Another 10 adults and 4 children under 10 years reported background pain at some reviews and not at others, including 2 adults and 3 children with RDEB-S (8 reviews), 6 adults and 1 child with RDEB-I (19 reviews), and 2 adults with RDEB-Inv (2 reviews).
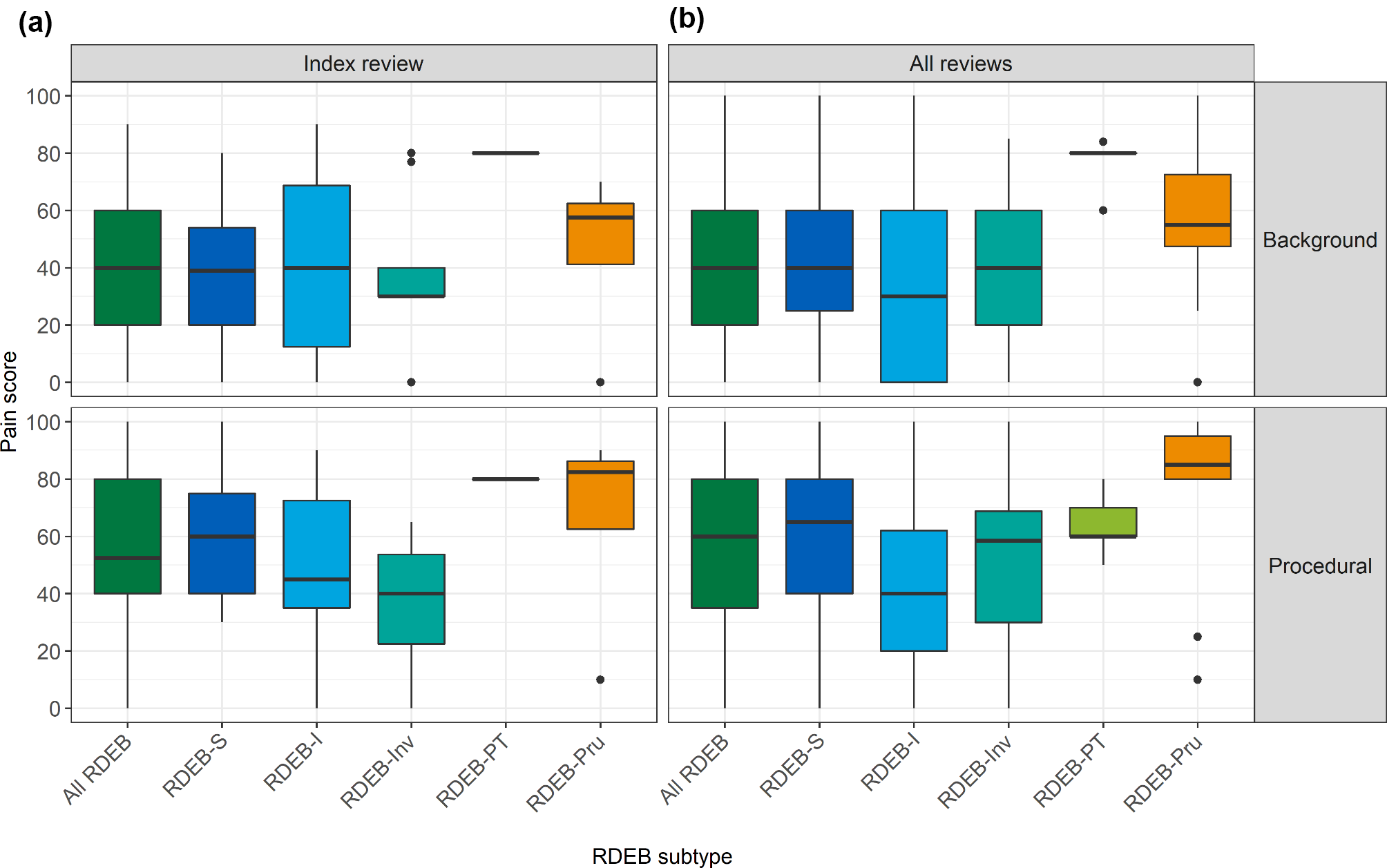
Table 3 Background and procedural pain VAS by RDEB subtype at index review (n = 61)Median background pain VAS at index review for all RDEB was 40 [20,60] out of 100, with RDEB-Pru reporting the greatest pain (Table 3; Fig. 1), and a similar pattern of background pain when all reviews were considered (Fig. 1, Supplementary Table 2). Background pain VAS scores at index review were positively associated with severity scores for all RDEB with medium to large effect size (Table 4). When considering all reviews, background pain VAS scores for all RDEB and for RDEB-I were moderate or strongly positively associated with iscorEB and BEBS severity scores, and weakly correlated for other subtypes (Supplementary Table 3).
Fig. 1
Box and whisker plot of background and procedural pain VAS at (a) index review (n = 61) and (b) all reviews (n = 361). Procedural pain VAS (n = 54) excluded participants reporting no/infrequent frequent dressing changes. Data reported in Table 3 and Supplementary Table 2
Table 4 Correlations between VAS background pain scores and severity scores by subtype at index review (n = 61)Median procedural pain VAS for participants reporting regular wound dressing changes at index review (n = 54) was 52 [40,80], which was a median 10 [0,21] points greater than reported background pain (Fig. 1; Table 3). At index review, individuals with RDEB-S and RDEB-Pru reported a distinct difference between procedural and background pain, 20 and 22 points, respectively, whereas those with RDEB-I and RDEB-Inv reported no difference (Table 3); the findings were similar when all reviews were considered (Supplementary Table 2).
Greater procedural pain at index review and when considering all reviews was positively associated with worse severity scores and longer time spent on dressing changes (Supplementary Tables 4 and 5). When considering subtype at index review, the only significant correlation was between procedural pain and iscorEB patient score (ISP) and iscorEB total score for RDEB-S and RDEB-I (Supplementary Table 4). For those with RDEB-S, pain was positively associated with BEBS scores with a 10-unit increase in BEBS increasing background pain by 5 points [95%CI: 1,9; p = .01] and procedural pain by 4 points [95%CI: 0,8; p = .04].
There was a large correlation between background and procedural pain at index review and adult QOLEB scores (and functioning and emotions subscores) for all subtypes except RDEB-Pru (Table 5). Similar results were observed for all reviews (Supplementary Tables 6 and 7). Thus, worse pain was associated with poorer QOL for adults. The relationship between parent and child QOL scores (PedsQL) and pain VAS varied widely and was difficult to interpret due to small review numbers (Supplementary Tables 6 and 7).
Table 5 Correlations between QOL and background and procedural pain scores by subtype at index review, adults only (n = 49)There were too few participants to explore differences in pain according to age at index review. However, when considering all reviews for RDEB-S, children under 10 years reported less procedural pain and their difference between background and procedural pain was smaller than for all other age groups; older participants with RDEB-S reported some pain at all reviews, whereas 4 (7%) child reviews with RDEB-S reported no background or procedural pain.
Frequency of painHalf the participants, 27 (55%) adults and 5 (56%) children, reported pain as ‘frequent’/’often’ or ‘constant’/’always’ at index review (Table 6). All adults and children with RDEB-S reported pain, whereas other subtypes reported greater variation in pain frequency. Supplementary Table 8 shows a similar pattern for adults (55%) when considering all reviews, although slightly less frequency for children (44%).
Table 6 Frequency of reported pain at index review by RDEB subtype (n = 61)One third of participants (38% index review, 37% all reviews) reported at least 4 nights disturbed sleep each week due to pain, with RDEB-Pru reporting the greatest disturbance (75% index review, 88% all reviews) (Table 6, Supplementary Table 8). However, one third of all RDEB reported no sleep disturbance (34% index, 34% all reviews), with a greater number of individuals with RDEB-I reporting no sleep disturbance in the previous month (55% index, 56% all reviews).
Location and intensity of painFigure 2 shows the variation in pain location and intensity when considering all reviews reported by different RDEB subtypes, with variation within and between subtypes (see also Supplementary Table 9). The most reported pain location was the skin, except for RDEB-Inv where mouth pain was more problematic. Individuals with RDEB-I reported lower pain frequency and intensity for each location, whereas those with RDEB-Pru reported greater intensity of overall pain, skin and bone/joints pain, although numbers were small and pain location did not correlate with any severity metrics. When outcomes were compared using the Mann-Whitney U test, with P-values adjusted using the Benjamini-Hochberg procedure, the only significant difference in pain location was between RDEB-S and RDEB-I, p = .026.
Fig. 2
Location and intensity of pain reported on iscorEB patient questionnaire when considering all reviews (n = 268). Data reported in Table 3 and Supplementary Table 9. Findings for index reviews cannot be reported as these early reviews retained only manual sub-scores so individual item scores not available for these
Moderate-large correlations for all RDEB were found between reported skin pain and BEBS score, likely due to severity of skin wounding (BEBS skin score), and dressing time (Supplementary Tables 10 and 11). Surprisingly, while there were significant correlations for milder subtypes (RDEB-I and RDEB-Inv), there were no significant correlations for those subtypes with greater wounding (RDEB-S and RDEB-Pru).
Treatment of painOne third of participants (31%) reported no pain medication usage at index review. Another 31% used regular and/or ‘as required’ (PRN) medication and 38% reported only PRN medication. Figure 3 (data in Supplementary Table 12) shows similar findings for median background and procedural pain VAS scores at index review and when considering all reviews for participants using different types of pain medication; many participants recorded more than one type of medication so may be reported more than once. Individuals of all subtypes using regular and/or PRN medication reported higher background and procedural pain VAS scores than those reporting only PRN medication (Supplementary Table 13). Individuals who did not report use of pain medication were more likely to report infrequent/no dressing changes than those using pain medication (21% vs. 7%) and also reported less annual dressing time (91 vs. 364 h), although these differences were not statistically significant. RDEB-S and RDEB-Pru reported the greatest strong opioid usage at index and all reviews (Supplementary Table 13).
Fig. 3
Pain medication usage at index review (n = 61) and all reviews (n = 361). Some participants reported using more than one type of medication. Data reported in Supplementary Table 12; Pain VAS, visual analogue scale measured from 0–100 mm
留言 (0)