The pathogenesis and manifestations of LN are heterogeneous and variable between and within individuals. Crescent formation is common in LN, especially in patients with a background of proliferative glomerular lesions. It was reported that the percentage of crescents was significantly associated with more severe kidney injury indices, such as the SLEDAI score, serum creatinine concentration, C3 value and several pathologically active indices [10]. Patients with “true” crescentic LN (affecting 50% of the glomeruli) had worse kidney outcomes than did those with pure class IV-G LN, which was also later confirmed by other investigators [11]. The recent development of a more accurate and reproducible histopathological classification system for LN is expected to lead to better disease categorisation. The field is moving towards more personalised treatment approaches.
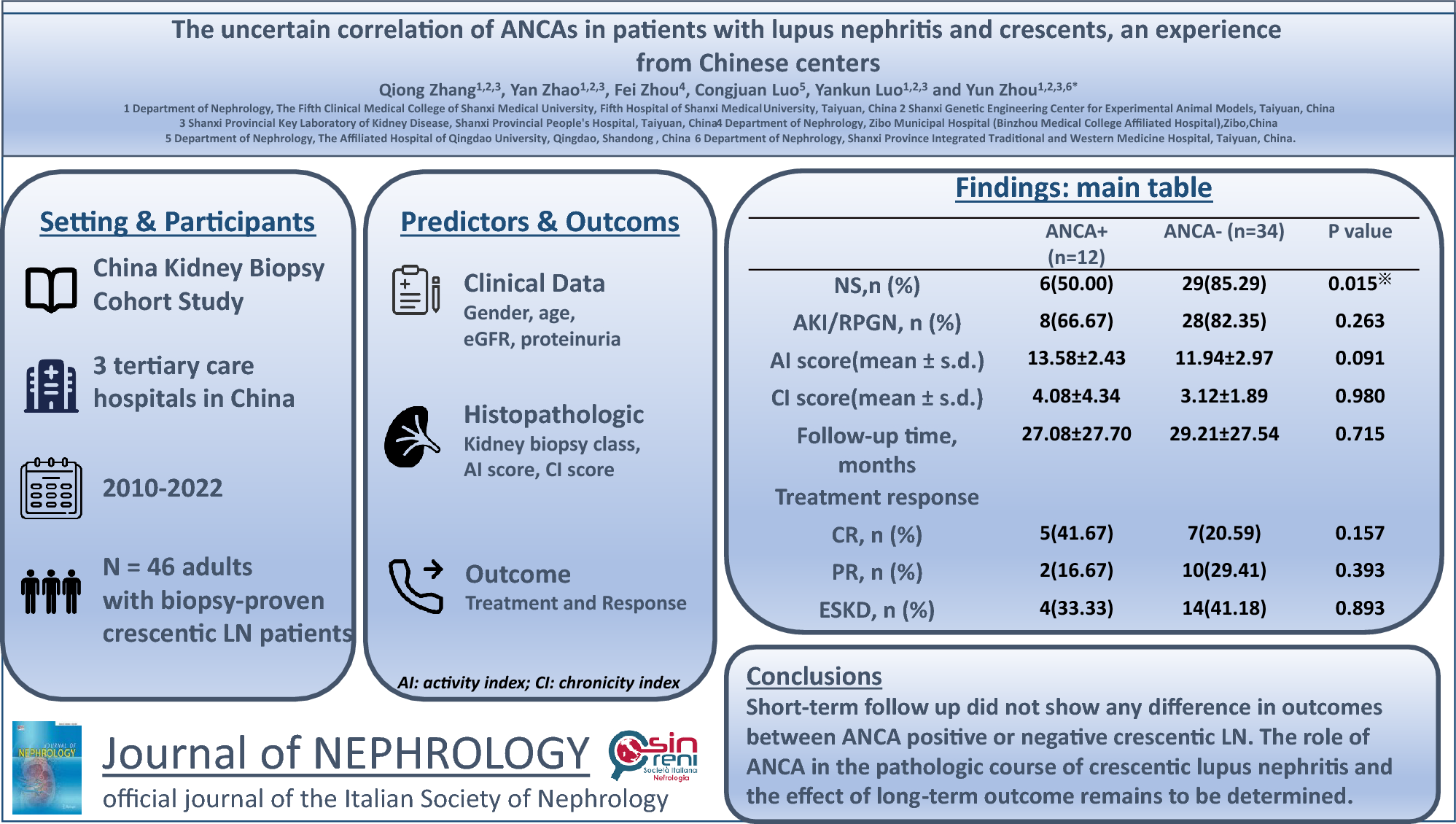
We found that crescentic glomerulonephritis was not rare in LN, accounting for 8.6% of the total biopsy-proven cases of LN. It was not surprising that patients with crescentic glomerulonephritis had a significantly greater incidence of acute kidney injury and clinical presentation, and worse outcomes. We found that 78.3% of crescentic LN patients presented with acute kidney injury and rapidly progressive glomerulonephritis, and 18/46 (39.1%) crescentic LN patients had developed ESKD at the last follow-up.
It has been reported that ANCA positivity rates range from 0 to 30% in LN [2, 4]. The role of ANCAs is unclear and debated [12]. Although most authors have indicated that ANCA seropositivity is common in patients with SLE, especially in those with disproportionate necrotising and crescentic features, several studies have failed to find a correlation between ANCAs and LN [13, 14]. The exact role of ANCAs in the pathologic course of crescentic LN has not been determined. In our study, ANCA positivity accounted for 18.8% of the total number of biopsy-proven crescentic LN cases. To investigate this phenomenon, we compared the clinical and pathological characteristics of patients who were and were not ANCA positive. We observed a significantly lower level of proteinuria, a lower proportion of nephrotic syndrome (p < 0.05) and a higher level of serum albumin (p < 0.05) in the ANCA-positive group than in the ANCA-negative group. Recently, several studies have shown that ANCA positivity may correlate with more haematuria, more proteinuria and higher creatinine levels [15, 16]. Other studies suggest that ANCA-positivity has no correlation with clinical indicators. We found that the urine protein level of ANCA-positive patients was lower than that of ANCA-negative patients and that the number of patients with nephrotic syndrome was lower. Moreover, the rate of acute kidney injury was not greater in ANCA-positive patients than in ANCA-negative patients. However, whether ANCA positivity is associated with SLEDAI score has not been determined [17]. We did not observe any differences in the extrarenal manifestations, C3 levels, SLEDAI values or serum ANA antibody positivity between crescentic LN patients with and without ANCAs. These results were not in accordance with most of the previously reported ones [2].
Positive ANCA antibody serology in patients with LN has been associated with distinct histopathological features on renal biopsy. It has been reported that patients with LN and positive ANCA serology are more likely to have segmental endocapillary hypercellularity and cellular fibroid crescents on renal biopsy (ISN/RPS Class III, IV-S, IV-G LN) [2, 4, 14] than are ANCA-negative patients. In our study, the total percentage of crescents was greater in the ANCA-positive group than in the ANCA-negative group; however, this difference in the proportion of total crescents in the glomeruli was not statistically significant. Moreover, there were no significant differences in the scores for cellular crescents, interstitial inflammation, tubular atrophy or interstitial fibrosis between the ANCA-positive and ANCA-negative groups.
It has been suggested that LN might facilitate the process of ANCA formation by promoting neutrophil degranulation and priming neutrophils, thus increasing the surface expression of ANCAs. However, the effect of ANCAs on the prognosis of patients with crescentic LN and on the remission rate has not been studied so far [18]. In our retrospective study, although the ANCA-negative group had a slightly greater incidence of acute kidney disease, there was no significant difference between the two groups. In accordance with our results, a study reported that there were no significant differences in therapy between LN patients with and without ANCAs [5]. Several recent studies have reported worse kidney survival in ANCA-associated vasculitis (AAV) patients. ANCA positivity is most likely related to smouldering disease, which causes ESKD [19]. Currently, there are rare reports on ANCAs and crescentic lupus nephritis. Abe et al. reported a patient with systemic lupus erythematosus who developed macrohematuria and massive proteinuria with pathological formation of fibrous crescents after seroconversion of MPO-ANCA, and suggested that tacrolimus might be a useful immunosuppressant for treating patients with progressive LN with MPO-ANCA [20]. We have summarised the clinical and pathological characteristics and clinical decision-making tendencies of previous ANCA and lupus nephritis in Table 4. Some studies have shown that rituximab was administered more frequently in ANCA-positive LN patients [21]. It was also reported that cyclophosphamide and mycophenolate mofetil might be useful for patients with progressive LN and MPO-ANCAs [2, 21]. Most studies have shown that there were no significant differences in therapy between LN patients with and without ANCAs [6, 20]. Further study of lupus pathology and ANCA subtype classification may be meaningful for the treatment of patients. However, we could not draw this conclusion from our study, and we observed no association between ANCAs and kidney outcomes in crescentic patients. There was no statistically significant difference in the initial treatment of immunosuppressants between the two groups. ESKD developed in 4/12 (33.33%) ANCA-positive LN patients and in 14/34 (41.18%) ANCA-negative LN patients in our study, but the difference was not significant. We showed that the percentage of ANCA-positivity was quite high in patients with crescentic lupus, possibly because of the formation of crescent-shaped LN. However, unlike what we assumed, based on our data, ANCA positivity did not seem to be related to disease activity, histopathologic features or kidney outcomes.
Table 4 The clinical, pathological relationship and treatment tendency between ANCA and lupus nephritisThe following factors may have contributed to our results. First, our data were obtained from lupus patients at three medical centres, and the sample size was small. Second, the detection method used for ANCAs may be nonspecific. In addition, ANCAs may not be the only antibodies involved, and some new markers are still under study. Third, the mean follow-up time for all our patients was 20 (6.75, 45) months. Most patients were followed up for less than 3 years, which may have affected the final results. Furthermore, all patients included in this study were of Chinese Han ethnicity.
In conclusion, ANCAs may be involved in the pathological changes observed in crescentic lupus nephropathy. However, ANCA positivity was not related to disease activity, histopathological features or short-term kidney outcomes. Within its limits, our study suggests that crescentic lupus nephritis with ANCA may not require a more aggressive treatment. However, further studies are needed to confirm this hypothesis.








留言 (0)