
記住我






Globally, the six major vIDPs—rabies, dengue, acute hepatitis, HIV/AIDS, EVD, and COVID-19—resulted in significant health burdens (see Table 1). In 2021, the total deaths due to vIDPs were approximately 8.7 million, and the DALYs were approximately 259.2 million, accounting for 12.8% and 9.0% of the global all-cause totals, respectively. Table 1 summarizes the deaths, DALYs, incidence, and prevalence associated with each vIDPs. In 2021, COVID-19 was the most impactful disease among those listed, with approximately 7.9 million (95% UI: 7.5, 8.4) deaths and 212.0 million (95% UI: 197.9, 234.7) DALYs. This stark contrast with other diseases underscores the unprecedented global impact of the pandemic. Additionally, acute hepatitis had the second highest age-standardized incidence rate at 3411.5 (95% UI: 3201.8, 3631.3) per 100,000 population, and HIV/AIDS had the second highest age-standardized prevalence rate at 483.1 (95% UI: 459.0, 511.4) per 100,000 population. Compared to 1990, the deaths and DALYs of acute hepatitis in 2021 decreased, while the deaths and DALYs of HIV/AIDS increased. Moreover, the deaths, incidence and prevalence of dengue has increased, with deaths rising from 14,315 (95% UI: 11,103, 18,652) in 1990 to 29,076 (95% UI: 17,628, 38,981) in 2021. Remarkably, the burden of rabies has significantly reduced, with DALYs in 2021 decreasing by 58.4% (95% UI: 44.8%, 71.9%) compared to 1990. Although the incidence and prevalence rates of rabies are relatively low, its high mortality rate continues to have a significant impact on the global disease burden. In comparison, the burden of EVD remains relatively low, with 48 (95% UI: 39, 56) deaths and 2602 (95% UI: 2130, 3062) DALYs in 2021. Figure 1 illustrates the global distribution of age-standardized DALYs rate for these diseases in 2021.
Table 1 Global burden of six viral infectious diseases of poverty in 2021 and 1990, with percentage change (numbers and rates)Fig. 1
Global distribution of age-standardized DALY rates for six viral infectious diseases of poverty for all ages and both sexes in 2021 (a rabies, b dengue, c acute hepatitis, d HIV/AIDS, e EVD, and f COVID-19). *The rate is per 100,000 population. DALY disability-adjusted life year. Map approval number: GS(2024)3052
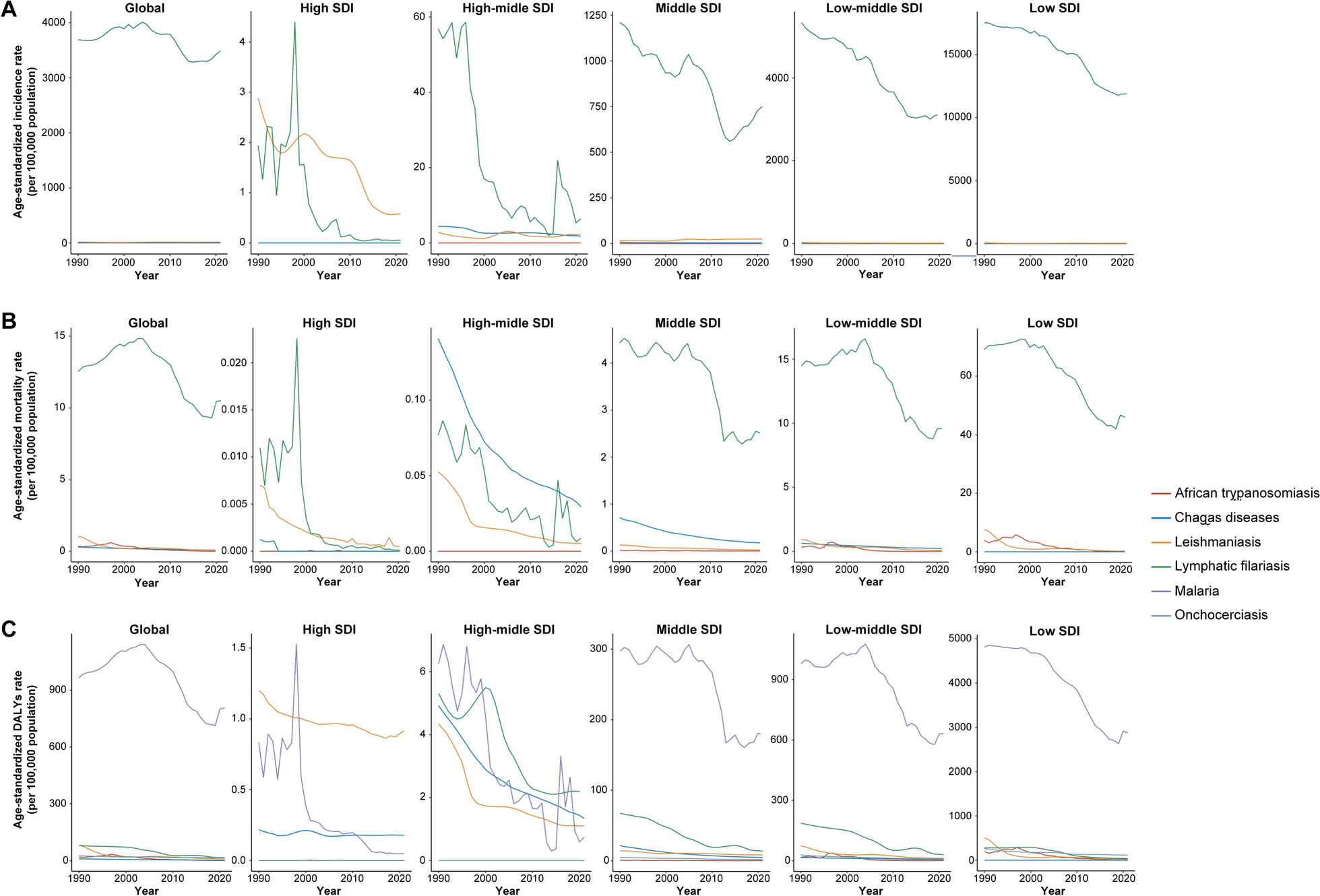
Trends by global and different SDI levelsThe trends depicted in Fig. 2 emphasize the dynamic and diverse impact of vIDPs globally and across different SDI contexts. From 1990 to 2021, the age-standardized DALY rate for HIV/AIDS peaked around 2003 at 1387.9 (95% UI: 1156.5, 1650.2) per 100,000 population globally, followed by a downward trend. However, in low SDI regions, HIV/AIDS continues to impose a significant burden, with age-standardized DALY rate remaining considerably higher than in other regions. COVID-19, which emerged at the end of 2019, rapidly escalated to become the leading cause of DALYs among the six diseases by 2021, demonstrating widespread impact irrespective of economic status. The age-standardized DALY rate for dengue initially increased, peaking in 2014 at 32.5 (95% UI: 20.5, 46.3) per 100,000 population. However, by 2021, it had only decreased to levels comparable to those around 2007, at 27.8 (95% UI: 14.2, 41.7) per 100,000 population. Particularly in low-middle and middle SDI regions, the disease continues to pose substantial challenges, with a considerable burden remaining as of 2021. Acute hepatitis and rabies exhibited relatively stable declining trends globally and across different SDI levels, with global reductions of approximately 68.0% (95% UI: 58.5%, 74.9%) for acute hepatitis and 69.4% (95% UI: 59.5%, 79.3%) for rabies in 2021 compared to 1990. Despite contributing to lower overall age-standardized DALY rates compared to other diseases, EVD showed notable spikes during specific outbreaks, particularly in low SDI regions.
Fig. 2
Trends in age-standardized DALY rates of six viral infectious diseases of poverty globally and by different SDI levels, 1990–2021. *The rate is per 100,000 population. DALY disability-adjusted life year; SDI Socio-Demographic Index
Age and gender differencesThe incidence rates and number of cases of vIDPs in 2021 exhibit distinct patterns across different age groups and genders, as shown in Fig. 3.
Fig. 3
Age and gender differences in incidence rates and number of cases of six viral infectious diseases of poverty in 2021 (a: rabies, b: dengue, c: acute hepatitis, d HIV/AIDS, e: EVD, and f: COVID-19)
For rabies, both the incidence rates and number of cases are relatively high among children and adolescents. The incidence rate is highest among the elderly, especially those aged 95 and above, with an incidence rate of 0.3 (95% UI: 0.2, 0.5) per 100,000 population. There is no statistically significant difference in the incidence rates and number of cases between males and females, with the total number of male cases being 6381 (95% UI: 3528, 8964) compared to 3800 (95% UI: 2202, 6184) in females.
For dengue, the incidence reaches its peak in the 10–14 years age group, with 6.3 million cases (95% UI: 1.5, 11.7). The incidence rate is also very high among those aged 95 and above, at 2768.8 (95% UI: 1012.7, 4885.7) per 100,000 population. Also, there is no statistically significant difference between males and females, with the total number of male cases being 27.3 million (95% UI: 6.0, 50.3) and 31.6 million (95% UI: 8.5, 56.6) in females.
Acute hepatitis shows a significantly higher risk of incidence among children and adolescents, particularly in children under 5 years old, with 77.8 million cases (95% UI: 70.4, 85.4) and an incidence rate of 11,815.5 (95% UI: 10,696.9, 12,969.7) per 100,000 population. Overall, the incidence rate among males in 2021 was significantly higher than among females, with males accounting for 3408.0 (95% UI: 3165.8, 3673.0) per 100,000 population and females accounting for 2946.1 (95% UI: 2754.0, 3153.8) per 100,000 population.
Young adults are the most affected by HIV/AIDS, with the incidence rate peaking in females at ages 25–29 years at 59.1 (95% UI: 51.6, 68.2) per 100,000 population, while the incidence rate for males peaks slightly later at ages 30–34 years at 59.8 (95% UI: 52.6, 67.5) per 100,000 population. Additionally, children under 5 years are another significant group affected by HIV/AIDS, with an incidence rate of 15.4 (95% UI: 12.8, 19.2) per 100,000 population. Among those aged 15–24, the incidence rate is significantly higher in females than in males. However, in the age groups 30–39 and 65–79, the incidence rate is significantly higher in males than in females.
The incidence of EVD is relatively low across all age groups, with a minor peak in children under 10 years and a more significant peak at ages 35–39 years, reaching an incidence rate of 2.0 (95% UI: 1.7, 2.2) per 100,000,000 population. The incidence rate decreases after age 40 but shows a slight increase again among those aged 75 and above. Overall, the incidence rate among females in 2021 was significantly higher than among males, with females accounting for 1.0 (95% UI: 0.9, 1.2) per 100,000,000 population and males accounting for 1.3 (95% UI: 1.2, 1.5) per 100,000,000 population.
For COVID-19, the highest risk of infection is observed among adolescents and young adults, particularly in the 15–19 years age group, where the incidence rate peaks at 36,557.6 (95% UI: 34,763.1, 38,238.8) per 100,000 population. The incidence rate decreases with age but shows an increase again among those aged 55 and above. This indicates that older adults face a higher risk of infection during the COVID-19 pandemic, possibly due to declining immunity and underlying health issues. Also, there is no statistically significant difference between males and females, with males accounting for 28,770.2 (95% UI: 27,525.9, 29,956.0) per 100,000 population and females accounting for 29,008.3 (95% UI: 27,764.9, 30,172.8) per 100,000 population.
Regional differencesIn 2021, in most regions, the global burden was highest for COVID-19, followed by HIV/AIDS, acute hepatitis, dengue, rabies, and lowest for EVD, as shown in Fig. 4. COVID-19 caused the highest DALYs in nearly all regions worldwide, underscoring its extensive impact. However, in East Asia, it ranked third with age-standardized DALY rate of 2.8 (95% UI: 0.8, 9.2) per 100,000 population. Sub-Saharan Africa bears the heaviest burden of HIV/AIDS, with DALY rates reaching 9615.8 (95% UI: 9003.0, 10,270.0) per 100,000 population, highlighting severe public health challenges. South Asia and Eastern sub-Saharan Africa show high DALY rates for acute hepatitis, with 140.3 (95% UI: 103.2, 197.4) and 129.0 (95% UI: 104.3, 163.0) per 100,000 population respectively. Southeast Asia exhibits a high DALY rate for dengue at 147.0 (95% UI: 95.3, 201.0) per 100,000 population. Rabies imposes a substantial burden in Eastern and Western sub-Saharan Africa, with DALY rates of 26.7 (95% UI: 10.3, 59.7) and 19.8 (95% UI: 7.9, 31.4) per 100,000 population, respectively. Central sub-Saharan Africa faces a significant impact from EVD, with a DALY rate of 1.1 (95% UI: 0.9, 1.3) per 100,000 population.
Fig. 4
Heatmap of age-standardized DALY rates for six viral infectious diseases of poverty by 21 regions in 2021. *The rate is per 100,000 population. DALY disability-adjusted life year
Table 2 presents the progress and ongoing challenges in managing the burden of major vIDPs across different regions over the past three decades. In both 1990 and 2021, Africa remained the region most severely affected by HIV/AIDS. Notably, while the burden in Eastern sub-Saharan Africa has decreased, it has significantly increased in Southern sub-Saharan Africa, with a percentage change of 225.0 (95% UI: 133.4, 343.9), and in Western sub-Saharan Africa, with a percentage change of 58.6 (95% UI: 18.5, 117.7). Additionally, the burden of HIV/AIDS has also markedly increased in Asia and Oceania. In contrast, the burden of acute hepatitis in 2021 showed a significant decline across all 21 regions globally compared to 1990, with a percentage change of − 68.0 (95% UI: − 74.9, − 58.5) globally. Meanwhile, regions such as Southeast Asia, South Asia, and Tropical Latin America have consistently been hotspots for dengue, continuing to exhibit high age-standardized DALY rates in both 1990 and 2021. Moreover, in high-income North America, while the overall burden of dengue remains relatively low, the DALY rate in 2021 showed a significant increase compared to 1990, with a percentage change of 427.1 (95% UI: 102.1, 1029.3). This rise suggests emerging threats and the need for vigilant public health measures to prevent outbreaks. Finally, globally, the DALY rate for rabies decreased by 69.4% (95% UI: 59.5%, 79.3%). However, in regions such as high-income North America, Western Europe, and Australasia, the burden of rabies increased significantly compared to 1990. This upward trend highlights the necessity for continued and enhanced rabies prevention efforts.
Table 2 Age-standardized DALY rates and percentage change for major viral infectious diseases of poverty in 1990 and 2021Relationship between vIDPs and SDIThe analysis reveals that the age-standardized DALY rates for vIDPs are all significantly negatively correlated with SDI, as shown in Fig. 5. Notably, there is a strong negative correlation between the DALY rates of acute hepatitis and SDI (r = − 0.8, P < 0.0001). Low SDI countries like Afghanistan show a significant disease burden, with DALY rates of 375.4 (95% UI: 251.6, 543.7) per 100,000 population. Similarly, rabies DALY rates also demonstrate a strong negative correlation with SDI (r = − 0.7, P < 0.0001). High SDI regions, such as high-income North America, Western Europe, and Australia, have DALY rates close to zero. In contrast, countries like Chad experience substantial disease burdens for both acute hepatitis and rabies, with acute hepatitis DALY rates of 178.9 (95% UI: 124.3, 254.0) per 100,000 population and rabies DALY rates of 22.8 (95% UI: 3.3, 59.4) per 100,000 population.
Fig. 5
Relationship between SDI and age-standardized DALY rates for six viral infectious diseases of poverty in 2021 (a: rabies, b: dengue, c: acute hepatitis, d: HIV/AIDS, e: EVD, and f: COVID-19). *SDI: Socio-Demographic Index; DALY: disability-adjusted life year
Furthermore, the analysis shows moderate negative correlations between the DALY rates of HIV/AIDS (r = − 0.6, P < 0.0001), COVID-19 (r = − 0.5, P < 0.0001), and dengue (r = − 0.4, P < 0.0001) and SDI. In regions with low SDI, such as Southern Africa, the burden of HIV/AIDS and COVID-19 remains high. For example, Malawi has HIV/AIDS and COVID-19 DALY rates of 6839.4 (95% UI: 5900.8, 8128.0) and 11,072.5 (95% UI: 9592.5, 12,394.8) per 100,000 population, respectively. Similarly, South-East Asia experiences high dengue DALY rates, with Indonesia having DALY rates of 279.8 (95% UI: 170.9, 404.4) per 100,000 population. In contrast, EVD shows a relatively weaker but still statistically significant negative correlation with SDI (r = − 0.2, P < 0.005).
留言 (0)