In the current study, we have proposed a novel approach for noninvasive testing to be utilized clinically for the prediction of DU in males with non-neurogenic LUTS, when differentiating from BOO. Our final model of good accuracy (c-index nearly 0.8) incorporated 10, both subjective and objective, factors of the following categories: free-flow curve shapes, uroflowmetry parameters, symptoms and symptoms’ severity assessed with the use of the CLSS questionnaire. These factors comprised fluctuating, fluctuating-intermittent and intermittent UFL curve shapes, lower PVR Ratio, less prevalent nocturia, more prevalent intermittency, less prevalent weak stream, lower straining points in CLSS, higher slow stream points in CLSS and higher incomplete emptying points in CLSS.
A particularly innovative aspect of our model is the incorporation of free-flow curve shapes, a parameter that has been explored in only few studies [9, 18]. We found that fluctuating curve shape, fluctuating-intermittent curve shape, and intermittent curve shape on the free-flow are predictive of DU, and not BOO. A study by Matsukawa et al. on males with non-neurogenic LUTS demonstrated results consistent with ours and showed that sawtooth and interrupted waveform curve shape on uroflowmetry are significant predictors of detrusor underactivity, distinguishing it from BOO [19]. Another study revealed that the prolonged/tailed shaped free urine flow curve patterns were independent predictors of BOO when differentiating from DU in female patients with voiding difficulty [18]. However, in our study only 4 patients with DU presented with prolonged curve shapes in UFL, rendering it non-diagnostic. Kocadag et al. compared flow rate curve patterns in female patients with LUTS and found that women without a prolonged void and bell-shaped traces had normal voiding urodynamics in 76% of cases, and the majority could be managed noninvasively. Patients with fluctuating and intermittent flow rate curves demonstrated a variety of urodynamic diagnoses, with a third of cases showing obstruction and a third showing detrusor underactivity. Plateau flow rate curve patterns were associated with urethral obstruction [9]. The aforementioned results underlined the significance of curve shapes in diagnosing the causes of LUTS in patients.
Another factor distinguishing DU from BOO in our model was the lower PVR Ratio (PVR-R). Rubilotta et al. introduced a novel functional parameter, the PVR Ratio, representing the ratio of post-void residual (PVR) urine to bladder volume (BV). Their study, using the ICS nomograms and BCI, revealed that median PVR-R and PVR were notably higher in obstructed and underactive males, compared to patients suffering from LUTS without BOO or DU [20]. Moreover, another study demonstrated that higher PVR-R was a significant predictor for BOO. However, the study compared patients with BOO to those without it, rather than specifically comparing DU to BOO [21]. Previous researches have investigated sheer PVR as a potential predictor of DU, however the results remain inconsistent. Our study did not identify PVR as a predictor of DU. Namitome et al. reported similar findings and demonstrated no significant difference in PVR and bladder voiding efficiency between patients with or without underactive detrusor [8]. Conversely, Jeong et al. observed a significantly increased PVR in male patients over 65 years old with LUTS and detrusor underactivity, compared to those with detrusor overactivity and bladder outlet obstruction [22].
Further variables included in our model encompassed the symptoms. Among these, we identified predictors of DU, as opposed to BOO, which included more prevalent intermittency, less prevalent weak urinary stream, less prevalent nocturia, lower straining score, higher slow stream score and higher incomplete emptying score on the CLSS questionnaire. In line with our findings, Gammie et al. observed a significantly higher prevalence of incomplete emptying and an interrupted urinary stream among patients with DU [7], aligning with our identification of intermittency and higher incomplete emptying score as predictors of DU in the current paper. Other research conducted by Çetinel et al. revealed that the presence of weak urinary stream was a significant predictor of BOO compared to DU and unclassified pressure-flow studies in females [18], a finding consistent with our observations in male population. However, the occurrence of weak urinary stream was also identified as a predictive factor for DU [8], when compared to all patients with non-neurogenic LUTS, such as overactive bladder, rather than solely when compared to those with BOO. Our analysis revealed that absence of weak stream in a patient is predictive of DU. However, if a patient already complains of weak stream, a higher slow stream score becomes a predictor of DU, indicating that if the weak stream occurs, it is more frequent and persistent compared to patients with BOO. A lower straining score was also indicative of DU in our study, suggesting that patients with DU tend to experience less straining, compared to those with BOO. This could be attributed to the nature of BOO, often involving an active obstruction below the bladder, which may require more additional abdominal pressure to overcome it. Additionally, the severity of the obstruction may fluctuate daily, which is potentially influenced by factors such as coexisting inflammation in the lower urinary tract, dietary habits, environmental factors, levels of physical activity and emotional stress or anxiety. However, research on this topic is currently very limited [23].
It is possible that the severity of lower urinary tract symptoms, rather than their sheer occurrence, plays an important role in distinguishing between DU and BOO. In this context, several studies on male population used mostly IPSS questionnaire [8, 24, 25]. However, we opted for the Core Lower Urinary Tract Symptoms score (CLSS) questionnaire proposed by Homma et al., as it is suitable for new patients, including those with multiple diseases, and without a definite diagnosis at first [13].
Our analysis identified less prevalent nocturia as a predictor of DU, a finding not confirmed by other studies distinguishing between DU and BOO [8, 25]. Nevertheless, this result appears plausible, given that the underactive bladder development may stem from damage to the bladder afferent and efferent pathways, or to the lumbosacral spinal cord [26]. Currently, significant emphasis is placed on neural mechanisms controlling the voiding process, particularly the afferent pathways responsible for monitoring bladder filling volume. The integrity of these pathways is crucial for the detrusor contraction efficiency. Therefore, any disruption to these nerves can lead to diminished bladder volume sensitivity, reduced detrusor contraction strength, or early termination of the voiding reflex. This can further impair voiding efficiency and result in hyposensitive bladder, leading to a lack of need to void at night [27], in contrast to an obstructed bladder outlet. This phenomenon may also account for disrupted bladder sensitivity during the day, and therefore higher incomplete emptying score that was also predictive of DU in our analysis.
In terms of urgency, previous studies indicated that less prevalent urgency was a predictive factor for DU when distinguishing it from BOO [8, 25], although this observation was not statistically significant in our study. The older age of patients included in these studies (median age = 70, IQR 65–76) and thus possibly more advanced damage to afferent and efferent bladder pathways, might potentially account for the discrepancy. Additionally, the study by Namitome et al. included patients with detrusor overactivity, present in 55% of cases [8], which could further explain the difference.
In our study, post-micturition dribble (PMD) was observed infrequently, with only 5 (3.9%) patients exhibiting this symptom in the DU group and 2 (2.0%) patients in the BOO group, rendering it non-diagnostic in our analysis. However, a study by Liu et al. demonstrated a correlation between PMD and voiding symptoms, along with an association with decreased Qmax. This suggests a need for further investigation, particularly among older men, as the study noted a significant increase in PMD prevalence with age [28].
It is important to acknowledge that symptoms constitute a subjective factor in the diagnostic process, lean solely on physician–patient dialogue, and demand comprehensive explanation of the medical terms followed by a meticulously taken medical history. This might explain why some studies have indicated that isolated symptoms classified by the International Prostate Symptom Score (IPSS) could not effectively differentiate patients with DU from those with BOO [10, 22], contributing to discrepancies between research findings in this regard.
Finally, in our study, age was not identified as a significant predictive factor for detrusor underactivity, contrary to other researches. These studies indicated an increasing prevalence of DU with advancing age [8, 22]. However, it is important to note that in these studies, the median age of patients was notably higher, with one study reporting a median age of 70 (IQR 65–76) [8] and the other study revealing that 63,8% of men were over 70 years old [22]. In contrast, the median age of patients in our study with DU is 61.5 (IQR 49–69.5), indicating a relatively younger population. This age distribution may contribute to the lack of statistically significant association between older age and DU diagnosis in our study. Moreover, the incidence of age-related comorbidities was low in our cohort. Statins were taken by only 4 (4.0%) patients in the BOO group and 6 (4.9%) patients in the DU group (Table 1). While age-related comorbidities associated with ischemia and oxidative stress, such as arteriosclerosis, are known to decrease detrusor contractility [27], they are not pertinent to our relatively youthful and healthy study population.
The calculated values for sensitivity, specificity, PPV, and NPV for our multivariate model were 75.8%, 62.4%, 71.9%, and 67.0%, respectively. These values are comparable to or slightly better than other DU predictors and diagnostic methods. Recently, Matsukawa et al. compared intravesical prostatic protrusion (IPP) between patients with detrusor underactivity (DU) and those with bladder outlet obstruction (BOO). They found that a lower IPP was a significant predictor of DU, with an optimal cut-off value of 8.2 mm yielding a sensitivity of 77% and a specificity of 73% [19]. Additionally, Matsukawa et al. identified bladder voiding efficiency (BVE) as a clinical predictor of DU, with a cut-off value of 70% providing a sensitivity of 73% and a specificity of 57% [19]. One study demonstrated that patients with DU had higher PVR compared to the control group, with a cut-off of 147 mL yielding a sensitivity of 60.16% and a specificity of 72.97% for diagnosing DU [24]. A novel study by Ishikawa et al. proposed serum adiponectin level as a DU predictor, with a cut-off value of 7.9 μg/mL providing a sensitivity of 79% and a specificity of 90% [29]. Although promising, serum adiponectin level testing is currently not widely available and remains costly.
Despite variations among studies concerning DU, we are confident that our newly developed model can be integrated into routine clinical practice, particularly during the initial ambulatory visit of patients. This is especially relevant in cases where non-adherence or potential lack of follow-up is suspected, or if a patient expresses reluctance towards undergoing an invasive pressure-flow study. Lastly, there is a high-risk group of patients, particularly those prone to infectious complications, who would greatly benefit if practitioners refrained from invasive tests during the primary diagnostics of LUTS. Conducting a comprehensive medical interview, coupled with the swift and easily applicable Core Lower Urinary Tract Symptoms score (CLSS) questionnaire, followed by a detailed analysis of the UFL curve and PVR volume, proves to be both time-efficient and cost-effective. This approach enables prompt initiation of appropriate medication, facilitating timely management of DU or BOO.
Limitations
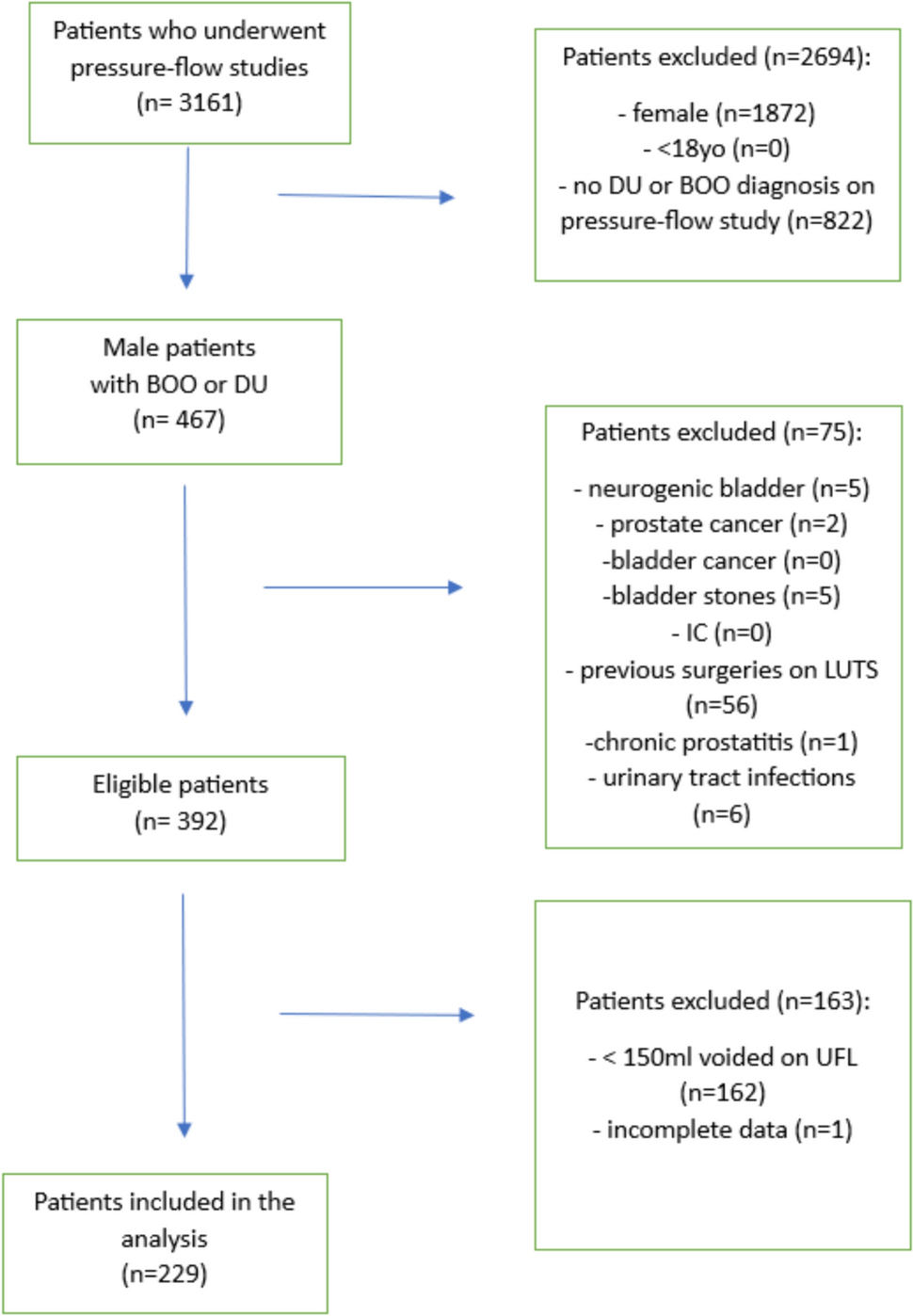
There are several limitations to our study that should be acknowledged. Firstly, this was a retrospective analysis, which may introduce biases and limitations inherent to its study design. Secondly, we excluded patients who could not void more than 150 ml on UFL, including those with urinary retention, which eliminated patients with severe voiding conditions and might have affected our results. Additionally, the patient cohort included in our study consisted of individuals with non-neurogenic LUTS suggestive of both BOO and DU, which does not represent the general population, as it was a single geographic and ethnic population study, performed on white Polish males. Therefore, the results obtained in our study are not applicable as a screening tool for a broader population or females. Furthermore, we did not evaluate prostate volume in our study participants, which could have provided additional insights into the relationship between prostate size and voiding dysfunction. Finally, some patients included in the study had already commenced medication affecting voiding patterns before undergoing noninvasive and invasive urodynamic testing.
Despite these limitations, we believe that our study provides valuable insight, particularly given the scarcity of research differentiating DU from BOO based on symptoms and noninvasive test parameters, without reliance on PFS outcomes. The findings of our study offer potential means to distinguish between DU and BOO in males using clinical examination and analysis of UFL parameters, especially in situations where PFS is unavailable or not accepted by patients. This insight seems most valuable when determining the appropriate treatment, whether noninvasive or invasive, such as transurethral prostate resection, in patients exhibiting symptoms indicative of BOO and DU. External validation of our model is warranted, considering other geographic and ethnic populations, to further explore its applicability and compare it with other existing models and diagnostic tools.


留言 (0)