
記住我





Eagle syndrome was first described in 1937 by Watt Eagle and is defined by the ossification of the stylohyoid ligament, which becomes abnormally long and may compress nearby vasculo-nervous structures, often presenting as cervicofacial pain. The length of the styloid process is typically 25–30 mm, and a length of >30 mm is considered elongated. The incidence of Eagle syndrome is approximately 4% in the general population, and only 4% of patients with Eagle syndrome exhibit symptoms (1). Another manifestation of Eagle syndrome is stylocarotid artery syndrome, a vascular variant of Eagle syndrome that can lead to neurological symptoms, including syncope, transient ischemic attack, or stroke (2). However, other atypical presentations have also been reported. This article aimed to review the literature to depict the characteristics of patients with the symptomatic vascular variant of Eagle syndrome.
Literature reviewA literature search was performed in February 2023 in the PubMed and Web of Science databases using the following keywords: (“Laminar cortical necrosis” OR “stroke” OR “brain vascular accident” OR “apoplexy”) AND (“Eagle syndrome” OR “stylohyoid syndrome” OR “styloid syndrome” OR “styloid-carotid artery syndrome” OR “elongated styloid process” OR “stylocarotid syndrome”), without time restriction.
A total of 31 and 35 articles were found in PubMed and the Web of Science, respectively. After removing duplicates, 36 articles remained. We excluded seven more articles because they were not relevant to our topic. The excluded articles were as follows: one article focused on a fracture of the styloid process found in a skeleton, another was about the prevention of vascular complications during neck surgery, four articles did not discuss any vascular complications, and the last article was a review of seizure-induced reversible brain MRI abnormalities in status epilepticus.
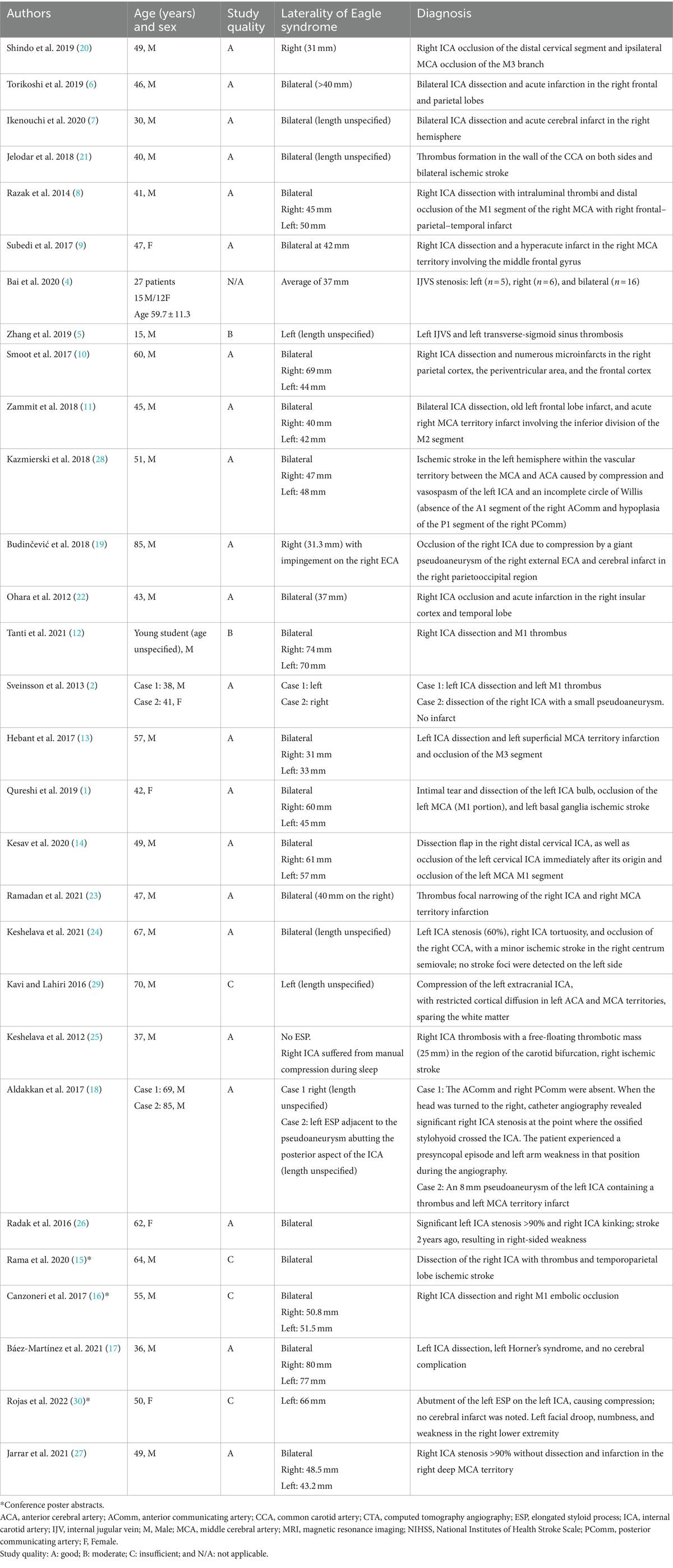
We analyzed the data from the remaining 29 articles, which are summarized in Table 1. The quality of the reported cases was assessed according to the criteria of the CARE checklist, which outlines the information to include when writing a case report (3). Quality was classified as good (when all key information was present in the article), moderate (when some non-major information was missing), and insufficient (when important information was missing). This classification was not applied to one article that presented aggregate data from a case series of patients (4). Of the remaining 28 articles, 22 were classified as good quality, 2 as moderate quality, and 4 as insufficient quality (3 of which were conference poster abstracts).

Table 1. Vascular variant cases of Eagle syndrome reported in the literature.
Vascular variants of Eagle syndrome are rare. The mean age of onset was observed to be 51 years (range: 15–85 years). The male-to-female ratio was 2:4, indicating a strong male predominance. In most cases (63%), the elongated styloid process (ESP) was bilateral. The ESP length involved in the vascular complications ranged from 31 to 77 mm, with an average length of 48 mm. Vascular complications were mostly represented by internal jugular vein (IVJ) stenosis (28 cases) (4, 5), followed by internal carotid artery (ICA) dissection (15 cases) (1, 2, 6–17). Eight cases of ICA thrombosis were also reported, two of which were caused by the formation of a pseudoaneurysm: one formed directly on the ICA containing the thrombus (18) and the other was due to indirect compression by a giant pseudoaneurysm of the external carotid artery (ECA) on the ICA (19). The mechanism of ICA thrombosis was not specified in the other cases (20–24). A particular case of a patient without an ESP who experienced right ICA thrombosis due to manual compression during sleep was reported (25). Two cases of severe chronic stenosis of the ICA > 90% involving the ESP were also reported (26, 27). Imaging findings typically observed in the ESP cases were mostly focal cortical infarcts due to embolization of the distal branches of the middle cerebral artery. Low carotid flow due to compression by the ESP was found in four cases in the literature, and laminar cortical necrosis as a cerebral complication of this compression was described in only one case. Kazmierski et al. (28) described the case of a patient with a junctional territory infarct between the left middle and anterior cerebral arteries caused by compression and vasospasm of the left ICA by the ESP. This patient had an incomplete circle of Willis, characterized by the absence of the A1 segment of the right anterior cerebral artery and hypoplasia of the P1 segment of the right posterior cerebral artery, which made it impossible for any arterial supply from the right ICA. Kavi and Lahiri (29) reported a similar case of laminar cortical necrosis in the left anterior cerebral artery and middle cerebral artery territories, caused by the compression of the left extracranial ICA by the ESP in a patient with a complete circle of Willis who had low blood pressure after hemodialysis, which made the arterial supply from the right ICA insufficient. Another remarkable case report highlighted the importance of postural involvement in the genesis of low blood flow caused by compression by the ESP (18). The patient experienced a presyncopal episode and left arm weakness when the head was turned to the right. Catheter angiography revealed significant stenosis of the right ICA where the ossified stylohyoid crossed the ICA. The last case was a poster abstract, in which a compression mechanism on the ICA by the ESP was described. However, we did not have enough information to establish this mechanism because the patient experienced bilateral symptoms with only the abutment of the left ESP on the left ICA. In addition, we did not have information about the circle of Willis or the circumstances of the neurological symptoms (30).
DiscussionVascular complications of Eagle syndrome are rare and may involve either the IJV, ECA, or ICA. These vascular complications may lead to cerebral ischemia due to either a thromboembolic mechanism or, less frequently, low blood flow, especially as a consequence of insufficient supply from the contralateral ICA in the context of an incomplete circle of Willis or low systemic blood pressure. Laminar cortical necrosis has also been rarely reported in patients with Eagle syndrome. This uncommon observation may be explained by the rarity of the syndrome itself and the specific circumstances required to provoke cerebral damage due to low blood flow, including a postural mechanism favoring the compression of the ICA by the ESP and an insufficient contralateral blood supply. Therefore, in such patients, other potential causes of laminar cortical necrosis must be considered. Laminar cortical necrosis is defined as focal or diffuse necrosis of one or more cortical laminae. The pathophysiology is linked to energy depletion, to which the gray matter is more sensitive than the white matter. It may be caused by a decrease in energy availability, as observed in stroke, hypotension, hypoglycemia, or mitochondrial disease, or by an increase in energy needs, such as in status epilepticus (31). Other factors that create an imbalance between energy needs and availability, causing laminar cortical necrosis, include endocrine, immunological, vascular, metabolic, infectious, toxic, or genetic etiologies.
In conclusion, although Eagle syndrome is rare, it should be considered in the diagnostic work-up of cerebrovascular events. Adequate imaging is thus required to visualize both the vessel lumen and adjacent anatomical structures.
Author contributionsJT: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. YB: Conceptualization, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
FundingThe author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interestYB reports personal fees from BMS, Pfizer, Medtronic, Amgen, Servier, NovoNordisk, Novartis, Boehringer-Ingelheim, outside the submitted work.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Qureshi, S, Farooq, MU, and Gorelick, PB. Ischemic stroke secondary to stylocarotid variant of eagle syndrome. Neurohospitalist. (2019) 9:105–8. doi: 10.1177/1941874418797763
Crossref Full Text | Google Scholar
2. Sveinsson, O, Kostulas, N, and Herrman, L. Internal carotid dissection caused by an elongated styloid process (eagle syndrome). BMJ Case Rep. (2013) 2013:bcr2013009878. doi: 10.1136/bcr-2013-009878
PubMed Abstract | Crossref Full Text | Google Scholar
3. Gagnier, JJ, Kienle, G, Altman, DG, Moher, D, Sox, H, Riley, D, et al. The CARE guidelines: consensus-based clinical case reporting guideline development. Headache. (2013) 53:1541–7. doi: 10.1111/head.12246
Crossref Full Text | Google Scholar
4. Bai, C, Wang, Z, Guan, J, Jin, K, Ding, Y, Ji, X, et al. Clinical characteristics and neuroimaging findings in eagle syndrome induced internal jugular vein stenosis. Ann Transl Med. (2020) 8:97. doi: 10.21037/atm.2019.12.93
PubMed Abstract | Crossref Full Text | Google Scholar
5. Zhang, F-L, Zhou, H-W, Guo, Z-N, and Yang, Y. Eagle syndrome as a cause of cerebral venous sinus thrombosis. Can J Neurol Sci. (2019) 46:344–5. doi: 10.1017/cjn.2019.17
Crossref Full Text | Google Scholar
6. Torikoshi, S, Yamao, Y, Ogino, E, Taki, W, Sunohara, T, and Nishimura, M. A staged therapy for internal carotid artery dissection caused by vascular eagle syndrome. World Neurosurg. (2019) 129:133–9. doi: 10.1016/j.wneu.2019.05.208
Crossref Full Text | Google Scholar
7. Ikenouchi, H, Takagi, M, Nishimura, A, Yamaguchi, E, Koge, J, Saito, K, et al. Bilateral carotid artery dissection due to eagle syndrome in a patient with vascular Ehlers-Danlos syndrome: a case report. BMC Neurol. (2020) 20:285. doi: 10.1186/s12883-020-01866-2
PubMed Abstract | Crossref Full Text | Google Scholar
8. Razak, A, Short, JL, and Hussain, SI. Carotid artery dissection due to elongated styloid process: a self-stabbing phenomenon. J Neuroimaging. (2014) 24:298–301. doi: 10.1111/j.1552-6569.2012.00759.x
PubMed Abstract | Crossref Full Text | Google Scholar
9. Subedi, R, Dean, R, Baronos, S, and Dhamoon, A. Carotid artery dissection: a rare complication of eagle syndrome. BMJ Case Rep. (2017) 2017:bcr2016218184. doi: 10.1136/bcr-2016-218184
PubMed Abstract | Crossref Full Text | Google Scholar
10. Smoot, TW, Taha, A, Tarlov, N, and Riebe, B. Eagle syndrome: a case report of stylocarotid syndrome with internal carotid artery dissection. Interv Neuroradiol. (2017) 23:433–6. doi: 10.1177/1591019917706050
PubMed Abstract | Crossref Full Text | Google Scholar
12. Tanti, M, Smith, A, Warren, DJ, and Idrovo, L. Internal carotid artery dissection due to elongated styloid process. BMJ Case Rep. (2021) 14:e245908. doi: 10.1136/bcr-2021-245908
PubMed Abstract | Crossref Full Text | Google Scholar
13. Hebant, B, Guegan-Massardier, E, Macaigne, V, and Triquenot-Bagan, A. Ischemic stroke due to internal carotid artery dissection associated with an elongated styloid process (eagle syndrome). J Neurol Sci. (2017) 372:466–7. doi: 10.1016/j.jns.2016.10.055
Crossref Full Text | Google Scholar
14. Kesav, P, Hussain, SI, Dogar, MA, and John, S. Stylo-carotid syndrome causing bilateral cervical carotid artery dissection requiring endovascular intervention. Clin Neurol Neurosurg. (2020) 195:105943. doi: 10.1016/j.clineuro.2020.105943
Crossref Full Text | Google Scholar
15. Rama, A, Xhaxho, S, Halili, G, Bilaj, F, Xhumari, A, and Kruja, J. A case report of eagle syndrome with carotid artery involvement. Int J Stroke. (2020) 15:523–3.
16. Canzoneri, C, Schroeder, A, Suarez, GC, and Gonzales, NR. A presentation of eagle syndrome as an etiology for carotid dissection and ischemic stroke. Ann Neurol. (2017) 82:S132–2.
17. Báez-Martínez, EM, Maure Blesa, L, Sobrino Guijarro, B, Ordoñez Gonzalez, C, Navas Vinagre, I, and García Torres, MA. Eagle syndrome. Pract Neurol. (2021) 21:548–9. doi: 10.1136/practneurol-2021-002949
Crossref Full Text | Google Scholar
18. Aldakkan, A, Dunn, M, Warsi, NM, Mansouri, A, and Marotta, TR. Vascular Eagle’s syndrome: two cases illustrating distinct mechanisms of cerebral ischemia. J Radiol Case Rep. (2017) 11:1–7. doi: 10.3941/jrcr.v11i8.3040
PubMed Abstract | Crossref Full Text | Google Scholar
19. Budinčević, H, Milošević, M, and Pavlović, T. Giant pseudoaneurysm of the external carotid artery causing stroke: a case report. J Clin Ultrasound. (2018) 46:269–72. doi: 10.1002/jcu.22524
PubMed Abstract | Crossref Full Text | Google Scholar
20. Shindo, T, Ito, M, Matsumoto, J, Miki, K, Fujihara, F, Terasaka, S, et al. A case of juvenile stroke due to carotid artery dissection from an elongated styloid process-revisiting conservative management. J Stroke Cerebrovasc Dis. (2019) 28:104307. doi: 10.1016/j.jstrokecerebrovasdis.2019.104307
Crossref Full Text | Google Scholar
21. Jelodar, S, Ghadirian, H, Ketabchi, M, Ahmadi Karvigh, S, and Alimohamadi, M. Bilateral ischemic stroke due to carotid artery compression by abnormally elongated styloid process at both sides: a case report. J Stroke Cerebrovasc Dis. (2018) 27:e89–91. doi: 10.1016/j.jstrokecerebrovasdis.2017.12.018
Crossref Full Text | Google Scholar
22. Ohara, N, Sakaguchi, M, Okazaki, S, Nagano, K, and Kitagawa, K. Internal carotid artery dissection caused by an elongated styloid process: usefulness of transoral ultrasonography. J Stroke Cerebrovasc Dis. (2012) 21:918.e7–8. doi: 10.1016/j.jstrokecerebrovasdis.2012.05.014
Crossref Full Text | Google Scholar
24. Keshelava, G, Kurdadze, R, and Tsiklauri, D. Surgical management of a patient with an internal carotid artery stenosis, eagle syndrome, and internal carotid artery tortuosity: a case of four pathologies of the carotid arteries. EJVES Vasc Forum. (2021) 50:37–9. doi: 10.1016/j.ejvsvf.2021.01.002
PubMed Abstract | Crossref Full Text | Google Scholar
25. Keshelava, G, Nachkepia, M, Arabidze, G, Janashia, G, and Beselia, K. Unusual positional compression of the internal carotid artery causes carotid thrombosis and cerebral ischemia. Ann Vasc Surg. (2012) 26:572.e15–7. doi: 10.1016/j.avsg.2011.08.020
Crossref Full Text | Google Scholar
26. Radak, D, Tanaskovic, S, Kecmanovic, V, Babic, S, Popov, P, and Gajin, P. Bilateral eagle syndrome with associated internal carotid artery kinking and significant stenosis. Ann Vasc Surg. (2016) 34:271.e15–8. doi: 10.1016/j.avsg.2016.01.015
PubMed Abstract | Crossref Full Text | Google Scholar
27. Jarrar, E, Naija, S, Grissa, O, and Amor, SB. Eagle syndrome: a rare etiology of ischemic stroke: a case report. Clin Neuroradiol. (2021) 32:869–71. doi: 10.1007/s00062-021-01096-0
Crossref Full Text | Google Scholar
28. Kazmierski, R, Wierzbicka, M, Kotecka-Sowinska, E, Banaszewski, J, and Pawlak, MA. Expansion of the classification system for eagle syndrome. Ann Intern Med. (2018) 168:746–7. doi: 10.7326/L17-0507
Crossref Full Text | Google Scholar
29. Kavi, T, and Lahiri, S. Teaching NeuroImages: eagle syndrome: cerebrovascular complications. Neurology. (2016) 87:e17. doi: 10.1212/WNL.0000000000002848
Crossref Full Text | Google Scholar
30. Rojas, E, Kaur, J, Gillenwater, S, Daya, A, Gandhi, A, Shekar, SP, et al. Eagle syndrome as a potential cause of hypoperfusion stroke: a case report. Am J Respir Crit Care Med. (2019) 199:A6642. doi: 10.1164/ajrccm-conference.2019.199.1_MeetingAbstracts.A6642
留言 (0)