This paper proposes a detailed characterization of AE and IE patients. We also developed a diagnostic tool to improve early diagnosis of encephalitis and hence accelerate adequate therapy in these patients.
Epidemiology and (para-)clinical patient characteristics
In our cohort, women and men were evenly represented. IE occurred approximately four times more frequently than AE, a reflection of the general incidence rates of these diseases [29,30,31]. Strict criteria were applied to ensure the inclusion of only those cases with a high level of confidence in the diagnosis of encephalitis and its classification as either IE or AE. In particular, unspecific syndromes accompanied by antibodies with low diagnostic value were excluded, as these cases are prone to overdiagnosis of AE [32, 33]. The distribution of AE subgroups is consistent with findings from other studies, with CASPR2, LGI1, and antibody-negative AE being the most frequently encountered entities in adults [30, 34, 35]. The spectrum of pathogens in IE reflects the regionality with a high prevalence of tick-borne encephalitis virus (TBEV), an entity with increasing prevalence due to global warming [36].
Most patients were hospitalized promptly after the onset of symptoms. However, some individuals—particularly in AE—presented only after a significant delay. In most of these cases, encephalitis was preceded by symptoms not easily recognized as signs of CNS inflammation, such as subtle faciobrachial dystonic seizures and depression, which may have been misinterpreted by both the patients and primary care physicians. The most common presenting symptoms were disorders of consciousness and cognitive deficits. This is unsurprising, as alterations of consciousness are included in the diagnostic criteria of the International Encephalitis Consortium, and cognitive impairments are considered a hallmark of AE [24, 37]. Additional symptoms, particularly acute symptomatic seizures, fever, and headache, have been found to effectively differentiate between AE and IE, with the former favoring AE and the latter two IE [29, 38]. Our study reaffirms their utility in distinguishing between the two conditions: a well-fitted model incorporating these as well as CSF pleocytosis/leukocyte count allowed for confident assignment of 93% of EUE cases to either IE or AE.
Focal neurological deficits were more prevalent in IE compared to AE. While AE commonly presents with the typical triad of limbic encephalitis, consisting of cognitive deficits, epileptic seizures, and psychiatric disorders, focal deficits are less frequent [37]. This may be due to the mesiotemporal pathology seen in many AE. The requirement for ICU treatment and mechanical ventilation was high in both patient subgroups. Some studies have linked these features to a poorer outcome [18, 39]. However, we did not observe a correlation with the overall outcome as measured by the mRS score. This unexpected result may have been influenced by a selection bias as multimorbid patients with severe encephalitis might not have been referred to intensive care in the first place.
Significant differences in laboratory parameters between AE and IE include CSF leukocyte count, as well as serum C-reactive protein (CRP), platelets, and sodium. In AE, reports have indicated either normal or only mildly elevated CSF leukocytes [12, 29, 31], with varying proposed cutoffs between 36 and 50 cells/µl to differentiate AE from IE [38, 40]. Lower serum sodium and platelets levels in IE compared to AE have been previously noted, possibly reflecting a more pronounced systemic reaction to infectious pathogens [29, 38]. These observations extend to clinical features such as headache and fever, which we found to be discriminative between the two conditions.
Characteristic MRI patterns are often absent in many cases of both AE and IE [31, 41]. However, among MRI-positive cases, there was a high prevalence of cortical and mesio-temporal lesions in AE. This can be attributed to the pathophysiology of AE, with limbic encephalitis ranking among the most common syndromes [37, 42]. Due to the high prevalence of TBE in our sample, basal ganglia and infratentorial lesions prevailed in IE [43].
Rates of encephalitis due to undetermined etiology remain high in various studies [29, 31]. Beyond the risk of introducing classification bias into research focused on this entity, this diagnostic uncertainty also proves challenging for clinical practice. Regarding our cohort, we were able to determine six discriminating factors that can easily be obtained early in the course of the disease: disorders of consciousness (favors IE), acute symptomatic seizures (favors AE), headache (favors IE), fever (favors IE), and CSF pleocytosis including leukocyte count (favors IE). On this basis, all but one EUE case could be assigned to either AE or IE. Bootstrapping was performed for internal validation of the discriminant analysis. Since the bootstrap confidence intervals are relatively wide, it is important to head the probabilities assigned to either IE or AE in the diagnostic tool and apply a clinical plausibility check, particularly when the probabilities approach 50% or the differential diagnosis concerns a highly unusual case.
Therapy and outcome
The therapeutic regimes administered to our patients adhere to the clinical practice guidelines on AE/IE [32, 44, 45]. The limited use of RTX may reflect the time of patient recruitment, as RTX has only recently been proposed as a treatment option in the initial therapy of severe AE. The add-on therapy with steroids and IVIG in IE may have been prompted by initial uncertainty regarding the pathogenesis of the encephalitis or could represent an anti-inflammatory approach to IE [46, 47].
Overall, the general outcome for patients with IE and AE was favorable, with 71% of all patients achieving an mRS of 0–2 at last follow-up (AE 66%, IE 73%). Within this group of patients with good outcomes, there was further improvement between initial discharge and last follow-up as deduced from a shift towards mRS scores of 0 and 1. These findings are consistent with previous reports indicating a favorable outcome in 80 to 100% of AE patients [39, 48] and approximately 50% in IE [49]. However, as we only included patients with a follow-up, initial mortality and morbidity is underestimated in our sample. Furthermore, the mRS does not capture the impact of neuropsychological and cognitive deficits on quality of life [42, 48, 50]. Hence, more specific encephalitis scores such as the CASE score or patient-reported outcome measures should be incorporated into studies on encephalitis outcome [51, 52].
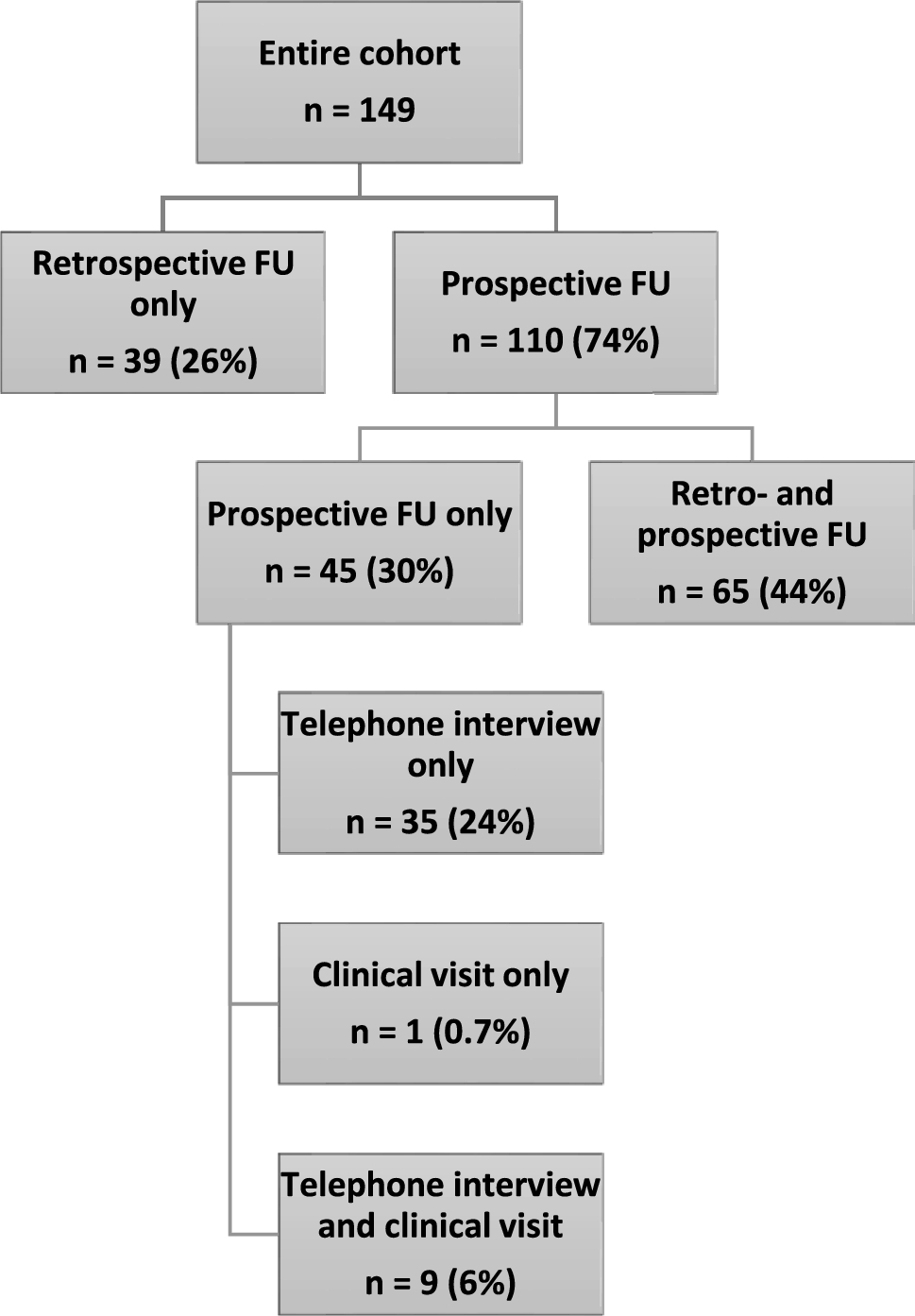
Advantages of our study include the large number of patients, the multicentric approach, and the opportunity for comparison of IE and AE characteristics and outcome within the same healthcare setting. Shortcomings of our study include the heterogeneity of our patient cohort concerning the causative pathology. This may have been further exacerbated by the extended recruitment and prolonged follow-up period which was partially due to the Covid-19 pandemic. While most patients had a prospective follow-up, only retrospective data were available in one quarter of the cohort. However, we still chose to include these patients to avoid bias towards patients with less severe clinical courses as among the main reasons participants could not be contacted prospectively were premature death or severe disability.
In summary, we present a comprehensive retro- and prospective analysis of the characteristics, outcome and differentiating factors of a sizable cohort comprising patients with AE and IE. Key findings from our investigation include:
Most frequent encephalitis etiology in an adult European cohort comprises seronegative and CASPR2-antibody-positive AE, and TBEV and S. pneumonia (IE).
Despite the often severe symptoms requiring ICU management, the majority of encephalitis patients experience resolution of focal neurological deficits and significant improvement in their activities of daily living (mRS) at hospital discharge compared to admission. Further improvement can be expected after hospital discharge.
We integrate six readily accessible clinical and CSF parameters (impairment of consciousness, acute symptomatic seizures, headache, fever, and CSF pleocytosis including leukocyte count) into a discriminative model for timely differentiation between AE and IE and provide a calculation tool for respective diagnostic probabilities. This tool will support clinicians in early decision making as to the therapeutic approach.






留言 (0)