
記住我






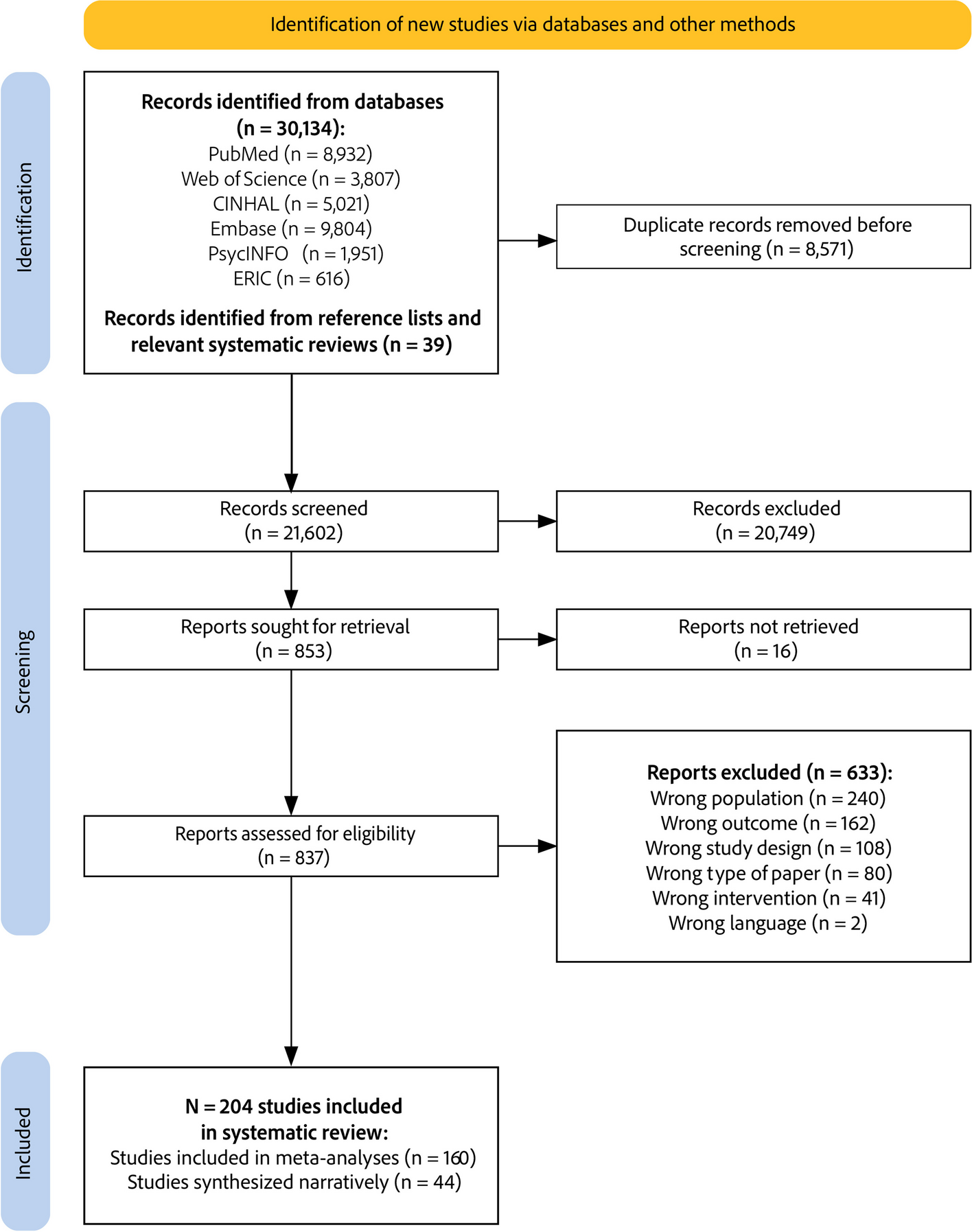
We identified 30,134 records from bibliographical databases and 39 from other sources, resulting in 21,602 unique records (see Fig. 1). Out of 837 records assessed for eligibility, 204 studies were included: 152 randomized studies and 52 controlled, non-randomized studies, enrolling 36,544 nurses (reported in 161 studies) and 340,320 patients (reported in 88 studies). All corresponding authors were contacted, and a total of 78 authors (38%) responded to requests for additional data. Out of the 204 studies included in the review, 160 contributed data to the meta-analyses for our primary outcome (compliance with desired clinical practice) and 44 were synthesized narratively.
Fig. 1
PRISMA study flow diagram
Characteristics of included studiesA summary of the characteristics of included studies is presented in Table 2. The majority were randomized studies (152 studies, 75%), including 96 CRTs (47%), 51 RCTs (25%), and 5 stepped-wedge CRTs (2%), involving a total of 30,473 nurses and 323,986 patients. Non-randomized studies accounted for 52 studies (25%), including 38 non-randomized controlled trials (19%), 13 non-randomized cluster-controlled trials (6%), and 1 controlled time series study (< 1%), involving 6,071 nurses and 16,334 patients. Most studies were conducted in hospital settings, particularly inpatient or emergency departments (139 studies; 68%). Primary care or general practice settings comprised 25 studies (12%), and nursing homes accounted for 21 studies (10%). Other settings included community health centers, homecare, hospital outpatient settings, public health units and skilled nursing facilities. In terms of country income status, most studies were conducted in high-income countries (160 studies, 78%), followed by upper-middle-income countries (37 studies, 18%), and a small number in lower-middle-income (7 studies, 3%) and low-income countries (1 study, < 1%). The studies targeted various clinical behaviors, with the most common focus on multiple behaviors (48 studies, 24%). Common behaviors included: providing counseling and advice (29 studies, 14%), infection prevention and control practices (26 studies, 13%), assessing and diagnosing illness (26 studies, 13%), administering medication (14 studies, 7%), documenting care (10 studies, 5%), and coordinating care (10 studies, 5%). Behaviors targeted in less than 5% of studies included testing and screening, managing physical restraints, managing symptoms, managing care equipment, prescribing, vaccinating, and reporting clinical incidents. Additional file 3 presents the characteristics of all included studies. Additional file 4 presents the excluded articles at full text assessment stage and reasons for exclusion.
Table 2 Summary of characteristics of included studies (N = 204)aRisk of bias across included studiesWe summarized the decisions regarding individual domains within the Cochrane RoB 2 tool and ROBINS-I in the risk of bias summary (see Fig. 2). Overall, for CRTs, the risk of bias for all outcome assessments (N = 227 from 96 CRTs and 5 stepped-wedge CRTs) was distributed as follows: 50% were assessed as low risk, 29% had some concerns, and 21% were considered high risk. For RCTs (N = 127 outcome assessments across 51 RCTs), 50% of the assessments were categorized as having some concerns, 28% as high risk, and 22% as low risk. For NRCS (N = 85 outcome assessments across 52 NRCS), 55% were considered to have a critical risk, 25% a serious risk, 18% a moderate risk and 2% a low risk. The full risk of bias assessment for each outcome, for RCTs, CRTs and NCRS is presented in Additional file 5.
Fig. 2
a Summary of risk of bias for cluster randomized trials. b Summary of risk of bias for randomized controlled trials. c Summary of risk of bias for non-randomized controlled studies
Use of implementation strategies across included studiesAs illustrated in the panel a of Fig. 3, among the implementation strategies employed in at least 10% of the studies, educational meetings were the most common (intervention arms [IAs] N = 155; control arms [CAs] N = 29), followed by educational materials (IAs N = 145; CAs N = 22), clinical practice guidelines (IAs N = 64; CAs N = 13), reminders (IAs N = 43; CAs N = 3), audit and feedback (IAs N = 38; CAs N = 1), educational outreach (IAs N = 32; CAs N = 1), tailored interventions (IAs N = 26; CAs N = 2), and local opinion leaders (IAs N = 24; CAs N = 3). Strategies employed in less than 10% of studies included patient-mediated interventions, local consensus processes, monitoring the performance of delivery of healthcare, clinical incident reporting, interprofessional education, communities of practice, managerial supervision, routine patient-reported outcome measures, educational games, and continuous quality improvement. No intervention used public release of performance data.
Fig. 3
a Frequency of use of each implementation strategy across intervention and control arms. b Frequency of combinations of implementation strategies in interventions assessed in included studies. EMeet = educational meetings, EMat = educational materials, CPG = clinical practice guidelines, R = reminders, A&F = audit and feedback, EO = educational outreach, TI = tailored interventions, OL = local opinion leaders, PMI = patient-mediated interventions, MPDH = monitoring the performance of delivery of healthcare, LCP = local consensus processes, CIR = clinical incident reporting, IPE = interprofessional education, COP = communities of practice, MS = managerial supervision, RPROM = routine patient-reported outcome measures, CQI = continuous quality improvement, EGames = educational games
As illustrated in the panel b of Fig. 3, implementation strategies almost always included some form of individual clinician education (including educational materials, educational outreach, and clinical practice guidelines) and/or group clinician education (including communities of practice, educational meetings, and interprofessional education) combined with reminders, audit and feedback, local opinion leaders, and tailored interventions. Additional file 3 presents the implementation strategies used across study arms.
Effects of implementation strategiesEffects of implementation strategies as a whole compared to no active interventionIn comparison with no active intervention, implementation strategies as a whole had significant positive effects on continuous clinical practice outcomes (76 assessments; SMD 0.94, 95% CI 0.72–1.15; I2 = 95%; see Fig. 4), and dichotomous clinical practice outcomes (60 assessments; OR 2.11, 95% CI 1.70–2.62; I2 = 95%; see Fig. 5). Statistically significant positive effects were also observed on nurses’ attitudes (30 assessments; SMD 0.59, 95% CI 0.23–0.95; I2 = 92%), knowledge (37 assessments; SMD 1.16, 95% CI 0.82–1.49; I2 = 91%), perceived behavioral control (19 assessments; SMD 0.74, 95% CI 0.35–1.13; I2 = 91%), and skills (10 assessments; SMD 0.97, 95% CI 0.42–1.52; I2 = 87%). No significant effects were observed on continuous patient outcomes (10 assessments; SMD 0.23, 95% CI -0.01–0.47; I2 = 87%) and dichotomous patient outcomes (12 assessments; OR 1.46, 95% CI 0.96–2.22; I2 = 84%). Statistical heterogeneity was high in all analyses. All forest plots are presented in Additional file 6. The clinical practice outcomes included in meta-analyses across all comparisons are presented in Additional file 7.
Fig. 4
Effects of implementation strategies on continuous clinical practice outcomes, compared with no active intervention
Fig. 5
Effects of implementation strategies on dichotomous clinical practice outcomes, compared with no active intervention
Table 3 presents subgroup analyses of the estimated SMDs for continuous outcomes and the estimated ORs for dichotomous outcomes to illuminate the variance in effects attributed to study design, study setting, and clinical behavior targeted for change. Minimal differences in effects were noted across these strata. Though, primary care/general practice for continuous clinical practice outcomes decreased and was no longer significant.
Table 3 Effects on clinical practice outcomes across strata for the primary comparison (any implementation strategy vs no active intervention)aEffects of specific implementation strategies on primary and secondary outcomesTable 4 displays effects of the implementation strategy subgroups by the primary outcome. Dichotomous clinical practice outcomes are positively affected (i.e., more likely to align with desired practice) by group clinician education, individual clinician education, reminders, patient-mediated interventions, tailored interventions, and opinion leaders. Continuous clinical practice outcomes are positively affected by group clinician education, individual clinician education, and tailored interventions. Across all implementation strategy subgroups, group clinician education, individual clinician education and tailored interventions had statistically significant effects on patient outcomes. These results may be influenced by heterogeneity and the lack of control over co-existing strategies within these subgroup analyses, likely leading to an inflation of the effects of individual strategies.
Table 4 Effects of implementation strategies on clinical practice and patient outcomes by subgroupTable 5 displays effects of the implementation strategy subgroups by secondary outcomes. Attitude (continuous) was positively influenced by group clinician education, individual clinician education, audit and feedback, and tailored interventions. Attitude (dichotomous) was positively influenced by group clinician education and individual clinician education. Knowledge was positively influenced by group clinician education, individual clinician education, and tailored interventions. Perceived behavioral control was positively influenced by group clinician education, individual clinician education, and reminders. Skills were positively influenced by group clinician education and individual clinician education. Perceived social norms were positively influenced by group clinician education.
Table 5 Effects of implementation strategies on the determinants of nurses’ behavior in clinical practice by subgroupEffects of multifaceted implementation strategies compared to single implementation strategyIn studies comparing a multifaceted implementation strategy (combining two or more implementation strategies) with a single type of implementation strategy, multifaceted strategies had small, non statistically significant effects on continuous clinical practice outcomes (12 assessments; SMD 0.23, 95% CI -0.01–0.46; I2 = 77%; see panel a of Fig. 6), dichotomous clinical practice outcomes (20 assessments; OR 1.35, 95% CI 0.76–2.40; I2 = 91%; panel b of Fig. 6), and dichotomous patient outcomes (5 assessments; OR 1.30, 95% CI 0.89–1.90; I2 = 0%) (see Additional file 6).
Fig. 6
Effects of multifaceted vs. single strategies on continuous (a) and dichotomous (b) clinical practice outcomes
Effects of implementation strategies in included studies not ineligible for meta-analysisAfter contacting all study authors, 44 studies were not included in meta-analyses for our primary outcome due to missing data (n= 27) [48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74], comparisons that were not relevant to our analyses (e.g., comparing two groups receiving the same type of implementation strategy with design variations) (n= 14) [75,76,77,78,79,80,81,82,83,84,85,86,87,88], or expressing their outcomes as rates rather than in a compatible format (n= 3) [89,90,91].
Of these studies, 25 focused solely on educational strategies, with 22 showing more favorable outcomes in the experimental groups. Kaner et al. [78] demonstrated that educational outreach increased brief alcohol interventions compared to clinical practice guidelines. Educational meetings (EMeet), often supplemented with educational materials (EMat) and/or clinical practice guidelines (CPG), led to improvements across various areas: blood glucose monitoring (O’Neill et al.: EMeet), [63] communication (Antonini et al.: EMeet), [48] diabetes management (Lim et al.: EMeet + EMat), [59] endotracheal suctioning practices (Day et al.: CPG + EMeet), [52] nursing documentation and care planning (Müller-Staub et al.: EMeet; Brady et al.: EMeet), [49, 81] use of physical restraints (Chang et al.: EMeet), [51] counseling (Tsai et al.: EMeet; Woodcock et al.: EMeet), [72, 86] and symptom management (Hessig et al.: EMat + EMeet; Michaels et al.: CPG + EMat + EMeet). [55, 61] Magnan et al. [80] used educational materials alone to improve physical examination. Nine studies evaluated technology-enhanced educational strategies. Carrico et al. [87] reported that biosimulated visual demonstration of particulate transmission resulted in increased personal protective equipment use. Jansson et al. [84, 92], through two studies, demonstrated adding feedback and debriefing to simulation-focused educational meetings, improved nurses' adherence to evidence-based guidelines for mechanical ventilation. Rutherford-Hemming et al. [82] found higher levels of evidence-based performance of neurological examinations in simulation-based education compared to a self-study module. Wang et al. [83] found improved application of counseling following the additional of simulation to educational meetings and materials. Wang et al. reported the effects of game-based learning on hand hygiene practices. [85] Kinsman et al. [88], Lau et al. [79], and Van de Steeg et al. [70] found e-learning programs improved physical examination, medication administration, and delirium care. Hammersley et al. [53], Seeley et al. [68], and Segal et al. [69] found no benefits from educational strategies.
Four out of five studies using audit and feedback alone were inconclusive. Charrier et al. [76] found that audit and feedback and the presence of facilitators, compared with self-monitoring, improved compliance to protocols for pressure lesions and the management of catheters. Bittner et al. [
留言 (0)