We first compared spirometry and PRM, two different methods of assessing small airways. The participants with SAD defined by both methods had similar clinical characteristics and a good overlap in different degrees of airflow limitation, but differed in airways and pulmonary vessels on HRCT. Our goal was to analyze predictive factors associated with the two diagnostic methods, explore the mechanistic differences between them, and provide insights for methodological advancements in SAD prediction.
A large cross-sectional study in China showed that the prevalence of SAD by spirometry was 43.5%, with older age, female gender, smoking, high BMI, and respiratory symptoms (including a history of chronic cough, childhood pneumonia or bronchitis) being risk factors [30]. In our cohort, the prevalence of SAD by spirometry was 31.4%, and by PRM was 40.7%. Similar to their findings, older age was also an independent risk factor in our study, aligning with the physiological loss of lung elastic recoil and terminal bronchioles associated with aging, which affects spirometry indicators [35,36,37]. Male gender was an independent risk factor for SAD in our research, and the BMI was lower in the SAD group. This could be attributed to the higher proportion of participants under 50 years of age in their study (48.2%) compared to ours (10%). In other related studies, SAD in younger populations was more likely associated with asthma, while high BMI was identified as a risk factor for asthma. Additionally, male gender and low BMI were found to be risk factors for COPD [38,39,40]. After multivariate adjustment, low BMI remained an independent risk factor for PRM-SAD in our study, which does not exclude the possibility of image noise alteration mediated by BMI, warranting further investigation.
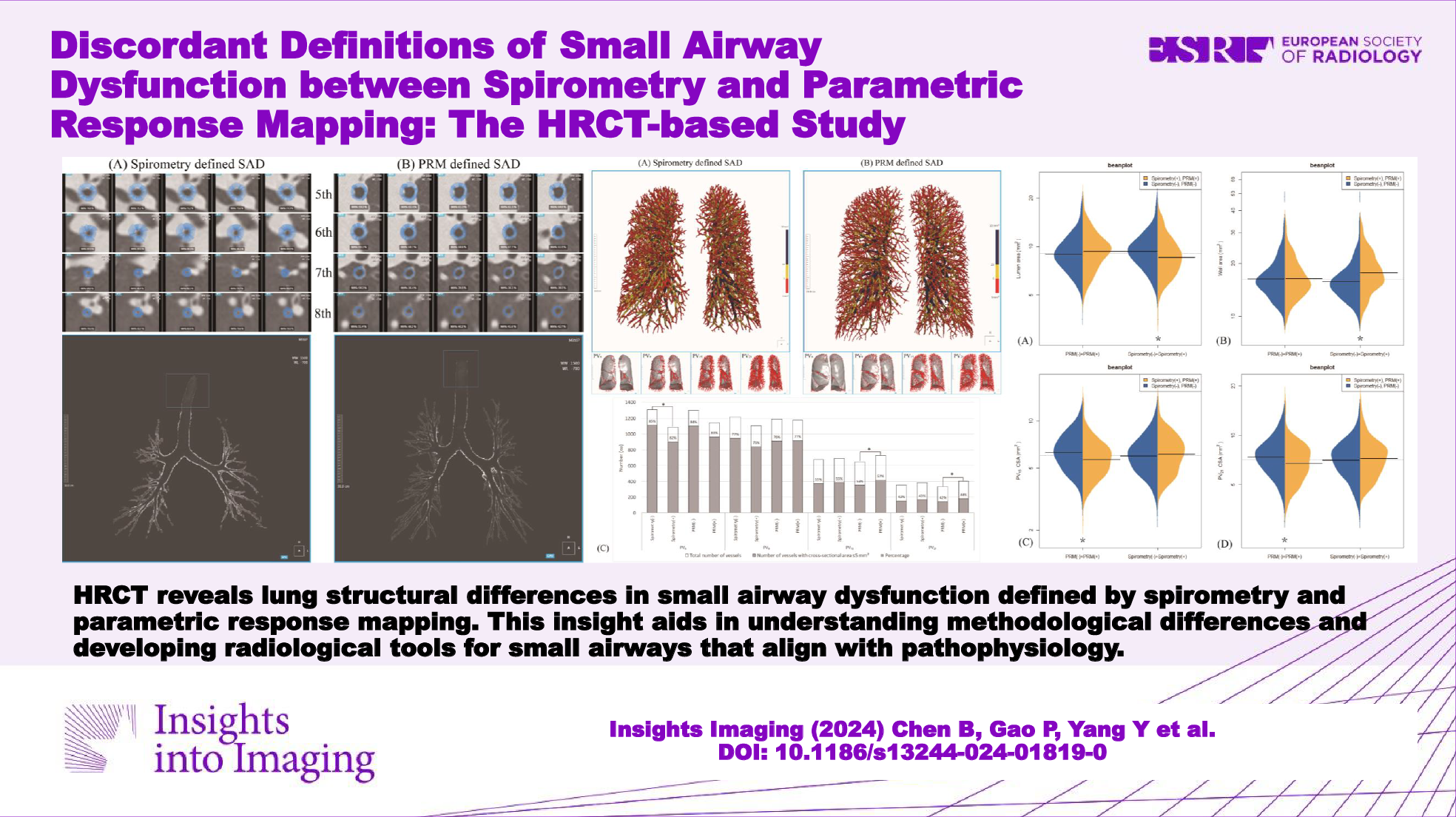
The small airways, often referred to as the silent zone of the lung, can develop functional impairments that are not easily detected. These impairments may occur due to environmental stimuli such as tobacco smoke, occupational dust exposure, and environmental pollution [38,39,40]. This impairment can gradually progress to irreversible obstructive lung diseases through various mechanisms [41,42,43] such as airway loss, wall thickening, mucus obstruction or alveolar attachment loss [1, 2, 4, 44]. Medium-sized airways are an extension of the small airways and can largely reflect the status of the small airways. In this study, HRCT showed that spirometry-SAD had reduced branch count, increased wall thickness and narrowed lumen, both at the whole lung level and the middle airway level (5–8 generations), consistent with the results of Lu et al [20]. Furthermore, branch count and visually assessed tree-in-bud sign and bronchial wall thickening on HRCT were independently associated with spirometry-SAD after multivariate adjustment, indicating a close relationship between spirometry and airway structure.
PRM-SAD had no obvious changes in airway structure at the whole lung level. However, subgroup analysis revealed that the Spirometry(−)PRM(+) showed the smallest WA% and the largest lumen, both at the whole lung level and at the 5th to 8th generation airway level. This finding fills the research gap between PRM and quantitative CT morphological relationships in medium-sized airways. Combined with the tree-in-bud sign as an independent risk factor, it suggests that PRM-SAD may be related to mucus obstruction and lumen dilatation, likely mediated by gas trapping. This contrasts with the observations of Vasilescu et al [12], who noted through micro-CT that PRMfSAD was associated with terminal bronchiole loss, lumen narrowing, and wall thickening. The possible reasons for this discrepancy might be that our study only measured airways at the intermediate level, and another reason could be that their study subjects were few and all had end-stage COPD.
Alveolar attachments are connective tissue septa linking airways and alveoli. Their loss reduces radial traction, causing premature airway closure and gas trapping during exhalation [44]. This early pathological change is observable even in pre-COPD patients without spirometry-detected airflow obstruction [5]. In quantitative CT, we analyzed medium-sized airway indicators on inspiratory CT, where the pressure difference inside and outside the airways increased. Early functional impairment shows that while the airway wall hasn’t significantly thickened, alveolar attachments are lost, yet the airway remains elastic, allowing significant lumen expansion during inspiration. This may relate to PRM-SAD morphological changes, such as reduced airway wall area and increased luminal expansion. Thus, PRM-SAD might indicate early alveolar attachment loss, warranting further research. Previous studies support PRM’s relation to alveolar attachments [12]. Additionally, PRMEmph is an independent correlate of spirometry-SAD in this study, consistent with other research [4, 45], suggesting SAD may precede emphysema. PRISm, a preclinical COPD state, was defined as SAD in 81% of cases in this study, with over half identified solely by PRM (Fig. 2). This demonstrates PRM’s sensitivity in assessing early small airway function. Further analysis of the correlation between lung histopathology in smokers or early obstructive pulmonary disease patients and PRM could yield more comprehensive conclusions.
Gas trapping impairs lung tissue gas exchange, causing local hypoxia, vascular proliferation, and wall thickening, while lung parenchymal destruction reduces the number of small pulmonary vessels [18, 46, 47]. In this study, HRCT showed that spirometry-SAD had thicker pulmonary vessels, possibly due to vascular smooth muscle hypertrophy in vascular remodeling [47]. However, PRM-SAD is characterized by thinner pulmonary vessels and a higher proportion of small vessels (CSA < 5 mm2), similar to Ritchie et al ’s findings [6], which showed a higher ratio of small pulmonary vessels in smokers compared to non-smokers, correlating with an accelerated decline in FEV1. This phenomenon might be due to more small vessels entering the scanner’s resolution range or gas trapping causing vascular constriction [48]. Additionally, thinner vessels and reduced blood perfusion could lower lung density, similar to the mosaic perfusion pattern seen on CT, potentially interfering with PRM’s gas trapping assessment. Although we analyzed lung parenchyma between −500 HU and −1000 HU to minimize the impact of airways and vessels on density [9], this measure could not completely avoid interference. Further research is needed to verify the cause-and-effect relationship between gas trapping and thinner pulmonary vessels. Additionally, BV1/TBV was a beneficial factor in the logistic regression model, indicating that a lower percentage of small vessel volume (CSA < 1 mm2) is more likely associated with PRM-SAD. This seems contradictory to the number of vessels with a CSA < 5 mm2, but it may relate to the lengths, numbers, and morphology of small pulmonary vessels beyond 21 mm from the pleura. Due to the complexity, further data and statistical analysis are required for interpretation.
Although PRM may be affected by the density of other lung structures due to its mechanism, various studies have shown that PRMfSAD correlates well with lung function indicators such as FEV1, FEV1/FVC, total lung capacity, alveolar volume, and residual volume [9, 10, 20]. In this study, it also overlaps significantly with spirometry-defined SAD at different GOLD stages and is more sensitive than spirometry in PRISm, thus reflecting small airway function to some extent. Future methods may better eliminate density interference from pulmonary vessels, airways, and lung interstitium. Based on this, combined with airway structure information, a three-dimensional spatial CT method conforming to pathophysiology could be developed for small airway assessment.
Our study also has some limitations. First, the attenuation value of voxels in PRM is affected by various factors. We have unified the CT scan parameters and reconstruction kernel, but the lack of respiratory gating may cause errors in gas trapping analysis [19]. In addition, our hospital is a comprehensive hospital with elderly characteristics, so the patients are generally older. We are planning to conduct a multi-center study to increase the sample size and diversity. Finally, the results lack histological evidence, because obtaining tissue samples is difficult, especially for early obstructive lung diseases.








留言 (0)